A clinical synopsis of the diagnosis and management of urinary tract infections
The part of the body responsible for the filtering, processing, and passing of liquid waste is known as the urinary tract. For clinical purposes, it is divided into the ‘upper’ urinary tract, which contains the kidneys and ureters (two thin tubes which carry processed waste liquid from the kidneys to the bladder); and the ‘lower’ urinary tract, which includes the bladder and urethra. It follows therefore that when we discuss urinary tract infections (UTIs), these are classed as upper or lower UTIs, dependent on location. After the lungs and inter-abdominal infections, the urinary tract is the second-most common bacterial infection site in the body.
There are primarily three types of UTIs, dependent on location:
- Cystitis (infection of the bladder) — a lower UTI.
- Urethritis (infection of the urethra) – a lower UTI and potentially more serious.
- Pyelonephritis (a kidney infection) – an upper UTI (ureters rarely would be a single site of infection).
UTIs have two classifications:
- Complicated — includes pregnant women, men, children, the elderly >65 and those with an upper UTI.
- Uncomplicated — those with lower UTIs, ie, acute dysuria (painful urination) or urinary frequency issues (either too often or not often enough) in females who are otherwise healthy, and men without a diagnosed upper UTI.
While UTIs can affect both genders of all ages, it is the most frequent bacterial infection identified in women, with females 30 times more likely than males to contract a UTI. Almost 50 per cent of women will experience an infection in their lifetime, with 30 per cent having their first occurrence by age 24.
Most of what is written, researched, and published on UTIs relates to women and children, which is natural as the lifetime occurance rate for men is only 12 per cent and most of these occur in men over 50 ( rare in <50 age group). This low figure for males, however, is deceiving as UTIs in men tend to be more complex, harder to diagnose and perhaps often indicative a more serious underlying condition.
When we consider children, UTI is the most common bacterial infection in the under- twos and in general terms, roughly 8 per cent of girls and 2 per cent of boys (more common in boys up to six months) will experience a UTI during childhood. Thirty per cent of children with a UTI will have a condition called vesicoureteric reflux, where urine flows back from the bladder to the ureters or in some cases the kidneys; for most, this is not a long-term condition.
In elderly people, UTIs can be harder to diagnose as the urinary system itself tends to weaken with age, especially in men. The existence of other comorbid conditions such as incontinence dementia can also hide the existence of a UTI.
CAUSES
In basic terms, UTIs are caused by the entry of bacteria ( from around the rectal or genital area) into the urethra. In many cases, the body can flush out the bacteria from the urethra before it spreads to other areas. When this doesn’t happen, the result is the bacteria beating the body’s defences and gaining a hold by spreading through infection to other parts of the urinary tract, ie, bladder, kidneys, etc. Other potential causes of UTIs can be:
- A blockage in the urinary tract, such as nephrolithiasis (kidney stones).
- Being sexually active — generally, a check for STI will be part of the diagnostic process for younger people.
- Diabetes or another condition which might compromise the immune system.
- Vesicoureteral reflux (as mentioned earlier – more common in children).
- Previous UTIs.
- Pregnancy.
- Difficulty voiding bladder (could be indication of underlying issue in men).
- Recent or current catheter use.
Anatomically speaking, women have a shorter urethra than men, so less distance for bacteria to travel, combined with the proximity of the urethra to the rectum, resulting in higher levels of infection of the bladder and kidney for women.
For pregnant women, their urine carries more proteins, sugars and hormones, which increases UTI risk. The growing baby can also put pressure on the bladder, which can prevent emptying the bladder completely, which also increases risk.
For men, as mentioned earlier, the risk of contracting a UTI aged under 50 is extremely low, however the risk increases with age as other male conditions such as enlargement
of the prostate (benign prostatic hyperplasia) can cause difficulty in emptying the bladder completely, or ‘turning off the tap’ (dripping) all present a significant increase in UTI risk. Prostatitis (inflammation of the prostate gland) is often associated with cystitis in men.
There is an increased UTI risk also for men who have had their prostate removed, as their urethra is also shorter due to surgery — so, again, less distance for bacteria to travel to urinary tract organs.
SYMPTOMS
Symptoms indicating a lower UTI (cystitis or urethritis) include:
- Increased urination frequency.
- Sudden need to urinate.
- Cloudy or smelly urine (may be indicative of dehydration and not a UTI).
- Burning feeling or pain when passing water.
- Feeling the bladder is not empty after urination.
- General sense of feeling unwell.
- Pain in lower abdomen.
It is important to note that a lower UTI can quickly develop into something more sinister, so, if any of these symptoms persist for more than a few days, or the person matches any of the statements below ,contact the GP.
- Male with UTI symptoms.
- Pregnant with UTI symptoms.
- Blood in urine.
- First time with a UTI.
- Symptoms persist following treatment. Symptoms of an upper UTI (pyelonephritis) may include, in addition to the above:
- Temperature of 38C or above.
- Chills and shivering or shaking.
- Pain in the lower back and/or sides. uConfusion and agitation (especially in older people).
- Feeling sick or has vomited.
- Diarrhoea.
Generally, someone presenting with any of these symptoms should contact their GP urgently as an undiagnosed kidney infection left untreated can be extremely dangerous.
If the person is very ill, they may need to be referred directly to hospital, especially:
- Elderly people, as there is a much higher risk of sepsis.
- Have cancer, diabetes, MS, or other serious medical conditions that could be compromised by severe infection.
In addition to the above, children may also: uWet the bed, especially in the case of the very young, where they have been consecutively dry for the previous few months — could be a sign of UTI.
- Wet themselves or deliberately avoid urination because it burns or stings.
- With babies, they may be irritable and not feed properly.
DIAGNOSIS
With any of the symptoms above, especially with children or upper UTIs, it is likely that the person will end up at the GP. As with any condition, getting an early diagnosis of the problem will help move quickly to the appropriate treatment and in most cases, as long as the treatment regimen has been followed, a successful outcome.
The doctor will ask questions to establish the nature and effect of symptoms and traditionally would take a urine sample to test. Urinalysis strips (dipsticks) are the most frequently used method to identify clinical evidence. For most women presenting with ‘typical’ symptoms of a lower UTI, ie, cystitis, urethritis, this test is usually sufficient to confirm a diagnosis and recommend a course of first-line treatment.
As a general rule, there are other circumstances where the doctor and recommended diagnostic pathway require the sample to be sent to the lab for further testing, including:
uAny case of UTI in men — this is to rule out other possible causes of symptoms, as UTIs in men are relatively rare by comparison.
- Any case where upper UTI is suspected. uUTI in pregnancy.
- Where there is blood in the urine — again, important to assess and rule out other causes, ie, bladder cancer.
- Where there is a higher risk factor present due to other conditions that may increase vulnerability to serious complications, ie, perhaps a diabetic with a weakened immune system.
There may be other factors where the GP considers further investigation, so other testing methods may be required, such as ultrasound. For example, an ultrasound can help assess early visual condition of kidneys and can also accurately measure ‘before and after’ bladder emptying volume. CT and MRI scans are other diagnostic options. A cystoscopy may also be recommended, where a tiny camera is inserted via the urethra to inspect the bladder, although ironically, this procedure itself carries a risk of UTI.
TREATMENT
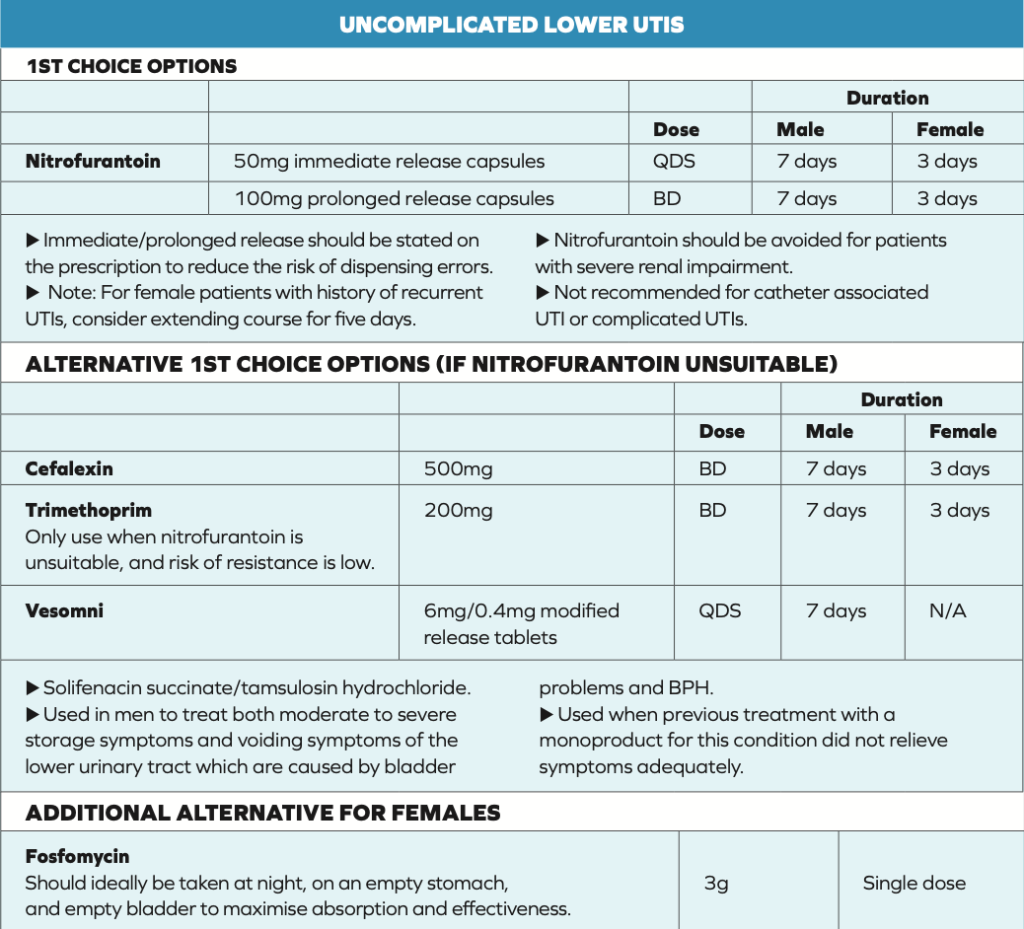
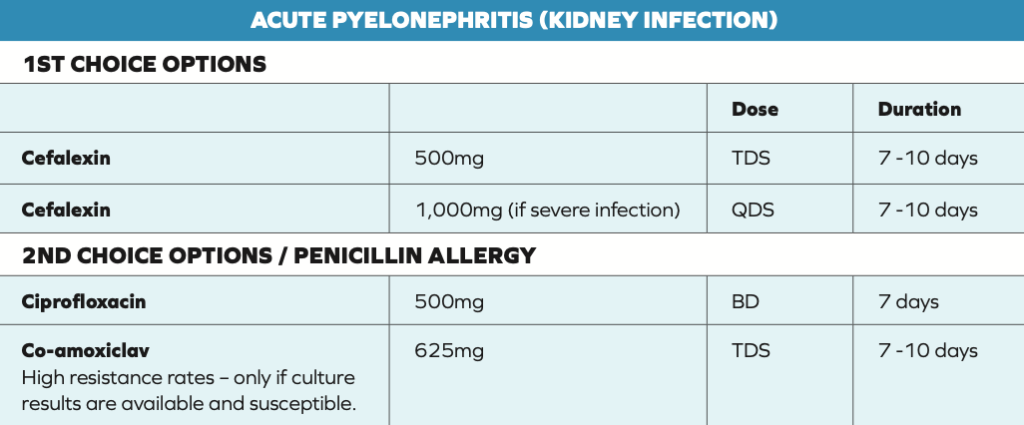
Once a UTI diagnosis is confirmed,in most cases a course of antibiotic treatment is prescribed. It is important to stress that the recommended course is completed, even if there is noticeable immediate improvement.
In terms of HSE prescribing recommendations, the last full review was in 2010, since when there has been a considerable amount of ambiguous and sometimes conflicting information on first-line treatment choices.
Following the most recent review in September 2021, the picture is a lot clearer, with standard treatment now being the same for both men and women for uncomplicated lower UTIs (more common); the only difference is duration of course. The table above shows what’s available according to the most recent recommendations.
SELF-HELP
When offering advice on how patients can help themselves prevent UTIs, consider the following Dos and Don’ts. DO
- Toilet hygiene — wipe from front to back — takes potential infectious matter away from urethra entrance.
- Fully void the bladder when urinating — minimises risk of urine remaining in bladder too long and infection risk.
- Drink plenty of fluids — helps in flushing out urethra regularly.
- Take showers instead of baths.
- Wear natural fabric underwear and loose-fitting jeans or trousers.
- Urinate as soon as possible following sexual intercourse.
- Maintain health cleaning routine for genitals.
DO NOT
- Don’t use perfumed hygiene products, soaps, bubble baths, etc.
- If you need to go, go! Do not hold it in. uAvoid contraceptive products with any spermicidal lubricant.
Regarding natural remedies, there is very little actual proof that cranberry juice or using probiotics or consuming natural yoghurt reduces the chances of contracting a UTI.
In summary, UTIs are all too common, especially for women. In a high percentage of cases, the infection is mild and can be managed with paracetamol or other OTC NSAIDs and other products available OTC that help reduce acidity of the urine and clear up in a couple of days. If symptoms do not improve within 48 hours, then it is important to keep close eye on any developing symptoms and take immediate action if things develop quickly.