






Dr Donna Cosgrove MPSI provides an overview of the importance of skin health, including the ageing process and the nutrients required for healthy skin
Introduction
Skin, the largest organ of the body, is made up of multiple layers. The epidermis forms an external barrier for protection while also facilitating secretion, absorption, filtration and excretion. There are
five epidermal layers: A horny layer (stratum corneum); a clear layer (stratum lucidum); a granular layer (stratum granulosum); a spinous layer (stratum spinosum); and a basal layer (stratum basale).
Beneath this is the dermis, which contains structures like capillaries, nerve endings
and hair follicles, sweat and sebaceous glands, along with fibroblasts that produce collagen, elastin, and glycosaminoglycans (GAGs). Under the dermis is the hypodermis, composed of adipose tissue, capillaries, and some additional cells and structures.1 The skin has multiple roles:
- It provides optimal conditions for deeper tissues by separating and protecting them from the external environment, ie, pathogenic microbes, chemical agents, mechanical/thermal factors.
- Maintains sufficient contact with the external environment to permit exchange of substances and receive stimuli.
- Regulates water and electrolyte balance (epidermal barrier and sweat glands).
- Thermoregulation.
- Sensory function.
- Metabolism, homeostasis, elimination, absorption and storage of substances.
Skin health and ageing
Ageing of skin is a natural and complex phenomenon due to genetic mechanisms and environmental factors such as UV radiation, cigarette smoke, and other pollution. There is an interplay between these intrinsic and extrinsic factors, closely linked to increased reactive oxygen species (ROS) and oxidative stress. The formation of ROS leads to protein and DNA damage, and amino acid racemisation, causing abnormal cross- linking of collagen and other structural proteins. Features of more mature
skin include wrinkles, loss of elasticity, pigmentation or discolouring, dryness, telangiectasias, foci of abnormal epidermal keratosis, and slower healing. Additionally, as we age, blood supply to the skin is reduced due to blood vessel degradation, leading to inadequate oxygenation and nourishment.1 Factors such as hydration, sebum content and surface acidity influence overall skin appearance (ie, texture, colour, physiological properties). Natural moisturising factor (NMF) in the stratum corneum, which consists of mainly amino acids, helps maintain adequate hydration and acidity levels. Essential fatty acids (EFAs) are required to both maintain the skin barrier and the integrity of the stratum corneum.
A balanced diet with essential nutrients is vital for the complex processes that take place in young and ageing skin. Skin — which has a high proliferative potential to allow for healing and growth — requires an adequate intake of proteins, fats and carbohydrates. There are anti-ageing ingredients in food, such as those that contribute to the synthesis and metabolism of skin components (peptides and EFAs) and those that inhibit degradation, such as substances that regulate enzyme expression (ie, matrix metalloproteases, MMPs).
Some skincare supplements like carotenoids and polyphenols may protect the skin from UV-induced effects due to antimutagenic, antioxidant and free radical scavenging properties. These include apigenin (found in many herbs, fruits and vegetables), quercetin (onion skin, apple peel), curcumin (turmeric), silymarin (milk thistle), genistein (soybeans), proanthocyanidins (grapes), and resveratrol (grapes, peanuts, red wine).
Certain vitamins and minerals are key elements for skin health Vitamin A and its derivatives, obtained from animal and plant sources, has a big impact on skin health. Plants contain beta carotene (a precursor to vitamin A), which is converted in the skin. Natural and synthetic retinoids can inhibit cell division during excessive proliferation, and activate it if the process has slowed. They also affect skin thickness and colour, regulate sebaceous glands, hair and nail growth, and affect melanin distribution.
The anti-ageing effects of retinoids are due to their influence on epidermal keratinocytes, dermal endothelial cells, and fibroblasts. Topical retinoids can penetrate the epidermis, and to a lesser extent,
the dermis and subcutaneous tissue. Retinoids contribute to the release of transcription and growth factors in the epidermis, and exfoliation of dead cells and proliferation of live cells in epidermal layers. They also reduce transepidermal water loss by strengthening the epithelial barrier. In the dermis, elastin and collagen synthesis is increased due to fibroblast stimulation.
All biologically active forms of vitamin A promote remodelling of reticulin fibres and capillary network synthesis in the dermis, and protect collagen from MMP mediated destruction, as well as inducing MMP inhibitors. Overall, this improves firmness, hydration and elasticity, with effects evident after 12 weeks of treatment.
Skin discolouration and pigmentation can be reduced by 60 per cent through application of topical retinoids through their influence on melanocytes and melanin distribution. Vitamin A and derivatives are used in the care of
Vitamin E includes
a group of lipophilic compounds and
is exclusively synthesised by plants
ageing skin, but also dermatological conditions which may be seborrhoeic (ie, acne, rosacea), viral, proliferative, cancerous, autoimmune (ie, lichen sclerosus), or papulosquamous dermatoses (ie, psoriasis).
Vitamin C concentration in the skin is higher than in other tissues.
It promotes the formation of the epidermal barrier and collagen in the dermis, protects against oxidation, helps counteract ageing, and is involved with cell growth and differentiation (involved with various skin diseases) via signalling pathways. Studies have shown that vitamin C enhances keratinocyte differentiation, resulting in stronger stratum corneum, which provides improved protection, and a higher vitamin C intake is linked to reduced wrinkles and dryness in older people.
Vitamin C is also responsible for the biosynthesis of collagen through its role in hydroxylation reactions, promotion of collagen gene and antioxidant enzyme expression,
and activation of fibroblasts, which increase collagen mRNA production. The antioxidant protection from vitamin C is limited to aqueous compartments, however, it reduces lipid oxidation by regenerating the fat- soluble vitamin E.
Topical vitamin C can counteract oxidative stress from UVA light, an effect enhanced when combined with vitamin E. Vitamin C is also thought to be involved in melangiogenesis inhibition. While melanin presence can help with photoprotection, an overproduction can result in hyperpigmentation diseases and initiation of melanomas.
Vitamin E includes a group of lipophilic compounds and is exclusively synthesised by plants. Alpha tocopherol is the most active form. This is transferred by Alpha-TTP (Alpha-Tocopherol Transfer Protein),
a crucial liver protein that specifically binds and transports alpha-tocopherol from the liver to the bloodstream and tissues, regulating the body’s overall vitamin E levels. Vitamin E can become a part of the lipid structures and protects against lipid peroxidation and skin ageing due to its free radical scavenging antioxidant properties, reducing DNA damage. It also reduces melanogenesis, which can help treat hyperpigmentation. Some studies suggest that vitamin E can play a role in aiding wound healing and treatment of atopic dermatitis, although there is conflicting evidence for the use of vitamin E to improve cosmetic appearance of scars.
Selenium, an essential mineral which is incorporated into enzymatic proteins, is important for skin function. It has a protective effect and can scavenge free radicals, protecting the skin against UV-induced oxidative stress. It can reverse UV light damage, and offer anti-inflammatory effects.
Zinc is present in all human tissues due to its importance in many physiological processes. The skin, particularly the epidermis, contains a high concentration.
Zinc has catalytic, structural and regulatory functions, including metabolism and gene transcription.
Its mechanism of action is linked to involvement in over 300 enzymes
and transcription factors, including antioxidant enzymes. Zinc is also essential for differentiation of new cells, and has roles in apoptosis and ageing. It stabilises skin cell membranes, maintains keratinocytes, and affects immune functions in the skin, such as modulating phagocytic activity and levels of inflammatory cytokines.
Oral and topical zinc administration has been used for its effect on skin regeneration and healing, with
pastes or ointments used to cleanse the skin of excess sebum, restore natural pH, and have astringent, anti-inflammatory and anti-acne properties. Zinc oxide is used as a physical filter in sunscreens due to its ability to reflect and disperse UV rays.
Copper is involved in many physiological and metabolic processes that are important for proper functioning of the human body. It also has a wide range of antimicrobial activity, both gram positive (ie, Staphylococcus aureus, Enterococcus faecalis, Clostridium difficile and Listeria monocytogenes) and gram-negative (ie, Escherichia coli, Pseudomonas aeruginosa and
Klebsiella pneumoniae) bacteria, fungi (including Candida albicans) and viruses (adenovirus, norovirus). In the skin, copper stimulates dermal fibroblast proliferation, and influences angiogenesis and the stabilisation of extracellular matrix skin proteins. Copper is a cofactor of superoxide dismutase, an enzyme that protects against free radicals. Copper is often used as an active component of face creams, but as with many active ingredients, the effectiveness is dependent on their ability to penetrate the skin.
Silicone is widely present in the body, including in the connective tissues, bone, liver, heart, muscles, kidneys, lungs, skin, hair and nails. Silicone plays a role in healthy skin structure, collagen production, strengthens connective tissue, reduces alopecia, promotes elastin and GAGs synthesis, and increases the resistance of nail and hair fibres, with concentrations decreasing as we age. Orthosilicic acid, which is the most bioavailable form of silicone, stimulates secretion of collagen from fibroblasts.
Essential fatty acids (EFAs) are among components of the intracellular structure that can limit transepidermal water loss, which helps ensure adequate hydration and protection. EFAs also have therapeutic properties such as anti- inflammatory and anti-allergic effects.
Symptoms of EFA deficiency include epidermal dryness, peeling, flabby skin, inflamed skin, increased skin irritation and slower healing.
Dermatology in community pharmacy
A survey2 of 174 pharmacy staff in the UK were asked to rank the order of frequency of seven skin conditions presenting in community pharmacy (Figure 1).
Additional skin conditions commonly encountered by staff included infectious diseases affecting the skin (ie, shingles, impetigo, chicken pox, hand foot and mouth, cold sores, athletes foot); reactions to external stimuli (ie, burns, UV damage, solar keratosis); dermatitis/eczema-related conditions (ie, seborrhoeic dermatitis); urticarias, erythemas and other inflammatory dermatoses (ie, hives, rosacea, urticaria); disorders of skin colour (ie, vitiligo, hyperpigmentation); disorders of skin appendages (ie, head and body hair loss); allergic reactions; skin lesions; skin cancer; boils; warts; verruca; corn; callouses and moles.
Survey respondents also gave the most challenging aspects of treating and managing people presenting in the pharmacy with skin conditions. The top five reported challenges were:
1. The ability to provide a differential diagnosis (69 respondents).
2. Knowledge of when and how to refer skin conditions (53 respondents).
3. Difficulties related to the availability of OTC treatment options (41 respondents).
4. Ability to choose and provide patients with the most appropriate treatment option (40 respondents).
5. Challenges in relation to the patient consultation, including challenges communicating when
using photos/telephone consultations, and challenges arising due to the sensitivity surrounding the topic of skin conditions (24 respondents).
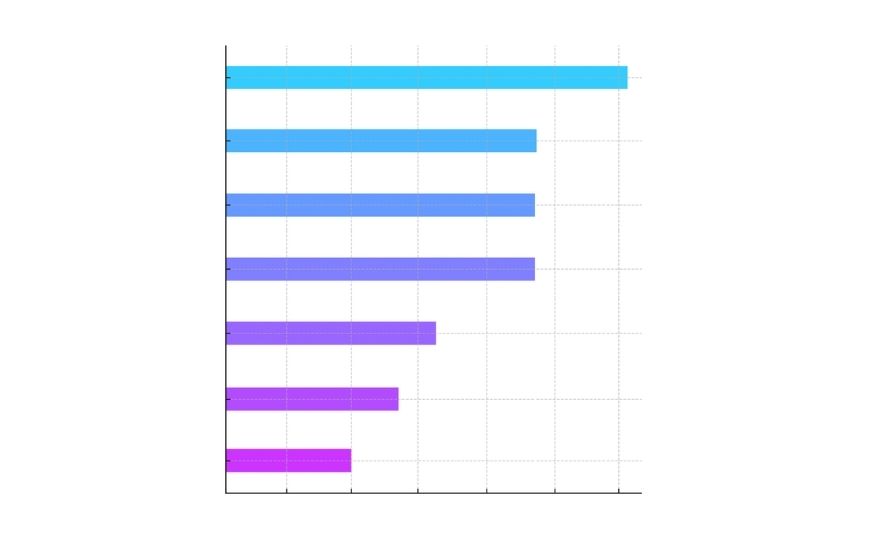
Figure 1: Commonly-encountered skin conditions seen by community pharmacy staff2
The authors suggest that greater support is needed for community pharmacy staff in provision of differential diagnosis, guidance on when to refer — including training resources that are inclusive of skin colour, and resources available for pharmacists to share with patients to support treatment information and adherence.
Skin health is governed by intricate structural, physiological and biochemical processes that are modulated by intrinsic ageing, environmental exposures, and nutritional status. Sufficient intake of essential vitamins, minerals and fatty acids is fundamental to the maintenance of epidermal
barrier function, optimisation of repair processes, and reduction of oxidative stress associated with ageing and pathological states.
A broad spectrum of dermatological conditions present in the community pharmacy setting, some of which may be appropriately managed with pharmacological interventions, others through specific nutritional optimisation, or a combination of both approaches.
Author: Dr Donna Cosgrove PhD. Donna’s overall aim is to improve patient outcomes through education. After graduating with a BSc in Pharmacy, she returned to university to complete a MSc in Neuropharmacology. This led to a PhD investigating the genetics of schizophrenia, followed by
a postdoctoral research position in the same area. She has worked in hospital, research and community pharmacy settings and is currently a community pharmacist in Galway and a clinical writer.
References
1. Michalak M, Pierzak M, Kr?cisz B, & Suliga E (2021). Bioactive compounds for skin health: A review. Nutrients, 13(1), 203. https://www.mdpi. com/2072-6643/13/1/203.
2. Shariff Z, Harvey J, Leighton P, Boyd M, Ridd M, Santer M … & Maidment I (2024). Perspectives of community pharmacy staff on commonly en- countered skin conditions and the key challenges towards enhancing their role in dermatology. Skin Health and Disease, 4(2), ski2-369.






