






COPD is a major cause of morbidity and mortality but correct treatment approaches can provide some relief, writes Eamonn Brady MPSI
Chronic obstructive pulmonary disease (COPD) is a progressive respiratory condition characterised by persistent airflow limitation, chronic respiratory symptoms such as dyspnoea (breathlessness), cough and sputum production, and recurrent exacerbations. It is most commonly caused by long-term exposure to noxious particles or gases, particularly cigarette smoke, although occupational exposures and environmental pollution also contribute.
The pathological changes seen in COPD include chronic airway inflammation, mucus hypersecretion, airway remodeling, and destruction of alveolar tissue, all of which contribute to irreversible airflow obstruction and impaired gas exchange.
COPD is a major cause of morbidity and mortality, both in Ireland and globally. It is associated with reduced quality of life, frequent hospital admissions, increased healthcare utilisation, and significant socioeconomic burden. Many patients live with undiagnosed or under-treated disease for years, during which lung function declines progressively. Earlier diagnosis and optimisation of treatment can improve symptom control, reduce exacerbations and improve long-term outcomes.
Community pharmacists are uniquely positioned to support people living with COPD. Through regular patient contact, pharmacists can identify patients at risk, optimise pharmacological treatment, reinforce inhaler technique, promote adherence, support smoking cessation, and encourage preventive interventions such as vaccination and pulmonary rehabilitation. As prescribing options and treatment pathways continue to evolve, pharmacists require up-to-date, practical knowledge of COPD management.
Previously in Irish Pharmacist magazine, I have written extensively about COPD, including the symptoms, causes, diagnosis, prognosis, etc. For this article, I concentrate on the treatment of COPD only. The focus is on pharmacist-relevant management of COPD, including inhaled therapies, management of exacerbations, add-on medicines, advanced and non-pharmacological treatments, emerging therapies, and prevention strategies.
Part 1: Bronchodilators and inhaled corticosteroids
Short-acting bronchodilator inhalers
Bronchodilator therapy remains the cornerstone of COPD management at all stages of disease. Short-acting bronchodilator inhalers deliver a small dose of medicine directly to the lungs, leading to rapid bronchodilation and symptomatic relief. In addition to improving airflow, these medicines reduce dynamic hyper- inflation, particularly during exertion, which is a major contributor to activity-related breathlessness in COPD.
There are two main classes of short-acting bronchodilator inhalers used in COPD. Short-acting beta-2 agonists, such as salbutamol and terbutaline, stimulate beta-2 adrenergic receptors in airway smooth muscle,
resulting in rapid relaxation and bronchodilation. Short-acting muscarinic antagonists, such as ipratropium bromide, inhibit acetylcholine-mediated bronchoconstriction by blocking muscarinic receptors. Both classes provide symptomatic relief within minutes of administration.
For patients with mild COPD symptoms, a single short-acting broncho- dilator used on an as-needed basis may be sufficient to relieve intermittent breathlessness. In some individuals, particularly those with preserved exercise capacity and infrequent symptoms, this approach may remain appropriate for a prolonged period. However, increasing reliance on rescue inhalers is an important marker of deteriorating disease control and should prompt review of maintenance therapy.
Historically, short-acting broncho- dilators were sometimes prescribed on a regular, scheduled basis. Current practice increasingly favours reserving short-acting inhalers for symptom relief and introducing long-acting therapy earlier in the disease course to improve overall control.
From a pharmacy perspective, monitoring refill frequency of short-acting bronchodilators provides a valuable op- portunity to identify patients with poorly controlled COPD and initiate medication review or referral.
Long-acting bronchodilator inhalers
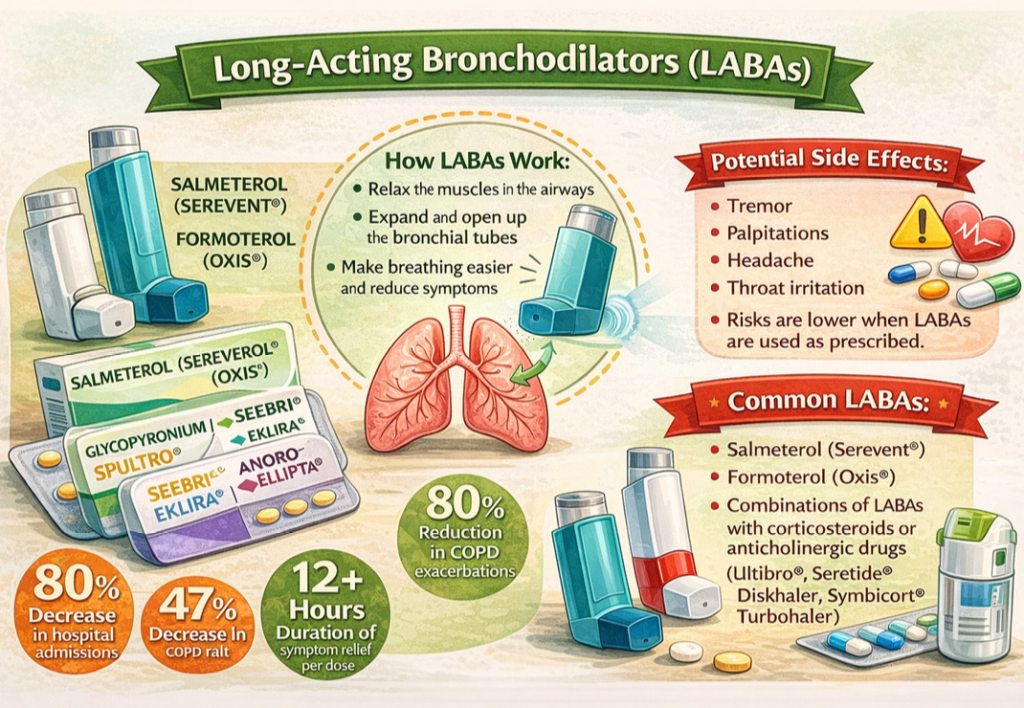
When symptoms persist despite short-acting therapy, long-acting bronchodilators are recommended. These agents provide sustained bronchodilation over 12-to-24 hours, improving lung function, reducing dyspnoea (breathless- ness), improving exercise tolerance and lowering the risk of exacerbations.
Long-acting beta-2 agonists include salmeterol, formoterol, indacaterol and olodaterol. Long-acting muscarinic antagonists include tiotropium, glycopyrronium, aclidinium and umeclidinium. Long-acting beta-2 agonist monotherapy is generally avoided in COPD, and beta-2 agonists are usually prescribed in combination with other agents.
Long-acting muscarinic antagonists are often preferred as first-line long-act- ing therapy due to their favourable effects on symptom control and exacerbation reduction. Extensive clinical evidence supports the effectiveness of anticholinergic long-acting therapy, particularly tiotropium, in stable COPD. Compared with ipratropium bromide, tiotropium is associated with improved lung function, fewer exacerbations, re- duced hospital admissions and improved health-related quality of life.
Inhaled corticosteroids in COPD
Inhaled corticosteroids (ICS) reduce airway inflammation but do not provide immediate symptom relief and do not slow the progressive decline in lung function seen in COPD. Their primary role is to reduce exacerbation frequen- cy in selected patients rather than to improve daily symptoms.
A short trial of inhaled corticosteroids may help distinguish asthma from COPD. Clear improvement in symptoms or lung function over several weeks suggests an asthmatic component. In COPD, inhaled corticosteroids are generally reserved for patients with moderate-to-severe disease who continue to experience frequent exacerbations despite optimised bronchodilator therapy, particularly those with raised blood eosinophil counts or features of asth- ma-COPD overlap.
Long-term inhaled corticosteroid use is associated with an increased risk of pneumonia, especially in older patients, those with low body mass index and those with advanced airflow limitation. Regular review of the ongoing need for inhaled corticosteroids is therefore essential, and withdrawal should be considered where risks outweigh benefits.
Combination inhalers and the role of the pharmacist Combination inhalers simplify treatment regimens and improve adherence by reducing the number of devices and daily doses required. Correct inhaler technique is critical to achieving optimal outcomes and should be assessed regularly. Community pharmacists are ideally placed to review inhaler technique, reinforce adherence, identify inappropriate duplication of therapy, and provide smoking cessation support.
Part 2: Newer combination inhalers and triple therapy in COPD
Over the past decade, the pharmacological management of COPD has evolved significantly, with increasing emphasis on combination inhalers. These inhalers combine two or more long-acting agents with complementary mechanisms of action, providing superior bronchodilation, improved symptom control and reduced exacerbation risk, while also simplifying treatment regimens and improving adherence. For many patients with moderate-to-severe COPD, combination inhalers now form the core of maintenance therapy and have largely replaced historical stepwise escalation approaches that relied on multiple sepa- rate inhalers.
Dual bronchodilator therapy (LAMA/LABA combinations) Dual long-acting muscarinic antagonist (LAMA) and long-acting beta-2 agonist (LABA) inhalers provide bronchodilation through two distinct and complementary pathways. By simultaneously inhibiting cholinergic bronchoconstriction and stimulating beta-2 adrenergic receptors, these inhalers achieve greater and more sustained airway relaxation than either agent alone.
Commonly prescribed LAMA/LABA combinations include glycopyrronium with indacaterol, tiotropium with olodaterol, umeclidinium with vilanterol, and aclidinium with formoterol. These in- halers are typically administered once or twice daily, depending on formulation.
Clinical trials consistently demonstrate that LAMA/LABA combinations result in greater improvements in lung function, reduced dyspnoea, improved exercise tolerance and decreased reliance on rescue inhalers compared with mono- therapy. Many patients experience clinically meaningful improvements in daily activities and quality of life.
Importantly, dual bronchodilator therapy also reduces exacerbation frequency in a significant proportion of patients. Unlike inhaled corticosteroid-containing regimens, LAMA/LABA combinations are not associated with an increased risk of pneumonia. This makes them particularly suitable for older patients and those with a history of recurrent chest infections. Current international guidance increasingly recommends LAMA/ LABA therapy as first-line maintenance treatment for symptomatic patients who do not have frequent exacerbations or features suggestive of corticosteroid responsiveness.
Selecting patients for dual bronchodilator therapy
Dual bronchodilator therapy is particularly appropriate for patients who experience persistent breathlessness despite monotherapy, have activity limitation related to dyspnoea, experience infrequent exacerbations, and do not have a history of asthma or raised blood eosinophil counts.
For pharmacists, patients transitioning to LAMA/LABA therapy often require additional counselling, particularly if a new inhaler is introduced. Reinforcing the distinction between maintenance inhalers and rescue inhalers remains essential to avoid inappropriate overuse of short-acting bronchodilators.
Inhaled corticosteroid and long-acting beta-2 agonist (ICS/LABA) combinations Combination inhalers containing an inhaled corticosteroid (ICS) and a long-acting beta-2 agonist (LABA) have a defined but more targeted role in COPD management. Examples include fluticasone furoate with vilanterol, fluti- casone propionate with salmeterol, and budesonide with formoterol.
ICS/LABA combinations have been shown to reduce moderate-to-severe exacerbations by approximately 20- to-30 per cent compared with placebo or bronchodilator monotherapy. The greatest benefit is observed in patients with frequent exacerbations, raised blood eosinophil counts or concomitant asthma or asthma-COPD overlap.
Long-term use is associated with an increased incidence of pneumonia, particularly in older patients, those with low body mass index and those with severe airflow limitation. Other adverse effects include oral candidiasis, dysphonia and potential systemic effects at higher doses. For this reason, ICS/LABA inhalers are no longer recommended as routine first-line therapy in COPD. Regular review is essential to ensure that patients receiving inhaled corticosteroids continue to meet criteria for their use. Pharmacists play a role in identifying patients who may no longer require ICS-containing therapy and supporting step-down or withdrawal in collaboration with the prescriber.
Single-inhaler triple therapy
Single-inhaler triple therapy combines a long-acting muscarinic antagonist, a long-acting beta-2 agonist and an inhaled corticosteroid in a single device. This approach is reserved for patients who remain symptomatic or continue to experience exacerbations despite optimised dual therapy.
Triple therapy has been shown to improve lung function, reduce exacerbation frequency and improve health-re- lated quality of life compared with dual therapy in selected patients. Benefits are greatest in those with frequent exacerbations and higher eosinophil counts.
However, as triple therapy includes an inhaled corticosteroid, pneumonia risk remains a consideration. Ongoing assessment of benefit versus risk is essential, and inappropriate continuation should be avoided.
From a pharmacy perspective, triple therapy simplifies treatment regimens but increases the importance of re- viewing medication histories to prevent duplication, particularly when patients are escalated from dual therapy without discontinuation of previous inhalers.
Inhaler devices, technique and adherence
The effectiveness of inhaled therapy depends not only on the pharmacological agent but also on correct inhaler technique and consistent adherence. Many patients with COPD struggle with device handling due to reduced inspiratory flow, arthritis, cognitive impairment or visual difficulties.
Community pharmacists should assess inhaler technique regularly, ensure that patients are using devices appropriate to their abilities, and provide tailored education. Poor technique and non-adherence are common contributors to poor disease control and avoidable exacerbations.
Part 3: Other medicines used in COPD
While inhaled bronchodilators form the foundation of COPD management, additional pharmacological options may be used in selected patients with persistent symptoms or frequent exacerbations despite optimised inhaled therapy. These medicines are generally reserved for individuals with more advanced diseases and require careful patient selection and monitoring.
Theophylline
Theophylline is an oral methylxanthine bronchodilator that has been used in the treatment of COPD for many decades. It exerts its effects through relaxation of airway smooth muscle, enhancement of diaphragmatic contractility, and improvement in mucociliary clearance. These mechanisms may provide modest improvements in airflow and symptom control in some patients.
In current practice, theophylline is used as add-on therapy in stable COPD when inhaled bronchodilator therapy has been optimised but symptoms persist. It is not effective for the management of acute exacerbations.
Antibiotics are indicated when patients present
with increased sputum purulence, increased sputum volume or worsening breathlessness
A major limitation of theophylline is its narrow therapeutic index. Therapeutic plasma concentrations are generally between 10 and 20mg/L, with adverse effects occurring at concentrations only slightly above this range. Common adverse effects include nausea, vomiting, headache, insomnia, palpitations and tachyarrhythmias. Severe toxicity may result in seizures or life-threatening arrhythmias.
Theophylline metabolism is influenced by numerous factors including age, hepatic impairment, heart failure, viral infections, smoking status and interacting medicines. Smoking increases the clearance of theophylline, while smoking cessation can result in a rapid rise in plasma concentrations, increasing the risk of toxicity. Regular plasma level monitoring is therefore essential, particularly following changes in smoking status or the introduction of interacting medicines. Due to its limited efficacy and safety concerns, other bronchodilator options are usu- ally optimised before theophylline is considered.
Mucolytic therapy
Mucolytic agents reduce the viscosity of respiratory secretions, making sputum easier to expectorate (cough up). In COPD, mucolytics may benefit selected patients with chronic productive cough, particularly those with chronic bronchitis and frequent exacerbations.
Commonly used mucolytics include carbocisteine and erdosteine. Evidence regarding their effectiveness is mixed; however, some studies suggest a modest reduction in exacerbation frequency and symptom burden in selected patients with moderate-to-severe disease. Mucolytic therapy should be reviewed regularly and discontinued if no clear clinical benefit is observed. Adequate hydration should be en- couraged alongside mucolytic use to maximise effectiveness.
Antibiotics in COPD exacerbations
Acute exacerbations of COPD are frequently triggered by respiratory infections, with bacterial pathogens such as Haemophilus influenzae, Streptococcus pneumoniae and Moraxella catarrhalis commonly implicated. Antibiotics are indicated when patients present with increased sputum purulence, increased sputum volume or worsening breathlessness.
Commonly prescribed antibiotics include amoxicillin, doxycycline and macrolides, selected according to local resistance patterns and patient-specific factors such as allergy history and previous antibiotic exposure.
Pharmacists should reinforce adherence to prescribed antibiotic courses and counsel patients on recognising signs of treatment failure or deterioration requiring urgent medical review.
Oral corticosteroids in exacerbations
Short courses of oral corticosteroids are a key component of COPD exacerbation management. Prednisolone at a dose of 30-to-40mg once daily for seven-to-10 days improves recovery time, lung function and symptom control, and reduces the risk of early relapse.
The benefits of systemic corticosteroids are greatest in patients with moderate-to-severe airflow limitation and significant inflammatory burden. Long-term systemic corticosteroid therapy is associated with significant adverse effects, including osteoporosis, glucose intolerance, hypertension, weight gain, cataracts and adrenal suppression, and should be avoided. Pharmacists should advise patients
to take corticosteroids in the morning with food and ensure appropriate gastroprotection where indicated.
Long-term macrolide therapy
Long-term prophylactic antibiotic therapy may be considered in patients with severe COPD and frequent exacerbations despite optimal inhaled therapy. Macrolides, particularly azithromycin, are most commonly used due to their combined antibacterial and anti-inflammatory properties.
Clinical trials have demonstrated reductions in exacerbation frequency and improvements in quality of life with long-term azithromycin therapy in selected patients. However, long-term use carries significant risks, including QT interval prolongation, hearing impairment, gastrointestinal adverse effects, and antimicrobial resistance. Baseline ECG and hearing assessment are recommended prior to initiation, and ongoing review is essential. Long-term macrolide therapy should be ini- tiated and supervised by a respiratory specialist.
Nebulisers and parenteral bronchodilators
Nebulisers may be used in patients with severe COPD or during acute exacerbations when inspiratory flow is inadequate for effective inhaler use. They allow delivery of higher doses of bronchodilators over a short period.
Intravenous aminophylline is now rarely used due to limited additional benefit and significant toxicity and is reserved for specialist settings.
Part 4: Advanced and non-pharmacological treatments
As COPD progresses, non-pharma- cological and advanced interventions become increasingly important in symptom management and prognosis.
Long-term oxygen therapy
Long-term oxygen therapy improves survival in patients with severe chronic hypoxaemia when used for at least 15 hours per day. There is no evidence of benefit in patients with mild or moderate hypoxaemia, and oxygen should not be prescribed solely for breathlessness. Smoking while using oxygen is extremely dangerous, and fire-safety counselling is essential.
Hospitalisation
Most exacerbations can be managed in the community; however, hospital admission may be required for severe breathlessness, hypoxaemia, hypercapnia, failure to respond to initial treatment, or significant comorbidities. In hospital, patients may receive controlled oxygen therapy, nebulised bronchodilators, systemic corticosteroids, antibiotics and non-invasive ventilation where indicated.
Lung transplantation and lung volume reduction Lung transplantation is reserved for carefully selected patients with end-stage disease and limited life expectancy. Lung volume reduction surgery and bronchoscopic lung volume reduction techniques may benefit selected patients with emphysema, improving symptoms and quality of life.
Part 5: Emerging and investigational therapies
Emerging therapies aim to modify dis- ease mechanisms and reduce exacerbations. Targeted lung denervation is an investigational bronchoscopic procedure designed to reduce parasympathetic bronchoconstriction and mucus secretion. Other experimental approaches include prostaglandin analogues, chymase-1 inhibition and stem cell-based regenerative therapies. These remain investigational and are not part of routine clinical care.
Part 6: Prevention and lifestyle measures
Smoking cessation is the most effective intervention to prevent COPD and slow disease progression at all stages. Pharmacists play a central role through brief interventions, phar- macotherapy recommendations and referral to cessation services.
Regular physical activity improves cardiovascular fitness, muscle strength and breathlessness. Pul- monary rehabilitation programmes provide substantial benefits, including improved exercise tolerance, reduced dyspnoea, enhanced quality of life, and reduced hospital admissions.
Optimal nutrition supports immune function and respiratory muscle strength. Adequate hydration helps maintain thinner respiratory secretions. Physiotherapy techniques such as breathing exercises and airway clearance methods may benefit selected patients. Annual influenza and pneumococcal vaccination reduce respiratory infections and exacerbations and should be actively promoted.
References
Global Initiative for Chronic Obstructive Lung Disease (2024) Global Strategy for the Diagnosis, Management and Prevention of COPD.
National Institute for Health and Care Excellence (2018) Chronic obstructive pulmonary disease in over 16s: diagnosis and management (NG115). Health Service Executive (2023) National COPD Clinical Programme.
British Thoracic Society (2022) Guideline for the management of COPD.
Celli, BR et al (2023). Pharmacological management of COPD. New England Journal of Medicine.
Wedzicha, J.A. et al. (2022) Prevention of COPD exacerbations. Lancet.
Calverley, PMA et al (2022). Inhaled therapies in COPD. European Respiratory Journal.
Vestbo, J et al (2023). Dual bronchodilation in COPD. Thorax.
Agusti, A et al (2024). Treatable traits in COPD. American Journal of Respiratory and Critical Care Medicine.
Lipson, DA et al (2023). Single-inhaler triple therapy. New England Journal of Medicine.
Suissa, S et al (2022). Inhaled corticosteroids and pneumonia risk. Chest.
Albert, RK et al (2022). Azithromycin for prevention of COPD exacerbations. New England Journal of Medicine.
Han, MK et al (2023). Non-pharmacological management of COPD. Lancet Respiratory Medicine.
Spruit, MA et al (2022). Pulmonary rehabilitation. European Respiratory Journal.
McCarthy, B et al (2023). Physical activity in COPD. Cochrane Database of Systematic Reviews.
Crisafulli, E and Clini, E (2022). Long-term oxygen therapy. Respiratory Medicine.
Valipour, A et al (2023). Bronchoscopic lung volume reduction. European Respiratory Review. Irish
Thoracic Society (2024). COPD standards of care in Ireland.
Written by Eamonn Brady MPSI (Pharmacist). Whelehans Pharmacies, 38 Pearse St and Clonmore, Mullingar. Tel 04493 34591 (Pearse St) or 04493 10266 (Clonmore). www.whelehans.ie. Eamonn specialises in the supply of medicines and training needs of nursing homes throughout Ireland. Email info@whelehans.ie






