






Eamonn Brady MPSI provides a synopsis of Crohn’s disease, including management and common complications
What is Crohn’s disease?
Crohn’s disease is one of the two main forms of inflammatory bowel disease (IBD), the other being ulcerative colitis. Crohn’s disease causes chronic inflammation of the gastrointestinal tract. Inflammation is the body’s natural response to injury or irritation and can lead to redness, swelling and pain. In Crohn’s disease, this inflammatory process is immune-mediated; however, it is not considered a classic autoimmune condition, as the immune system does not appear to be directly attacking healthy tissue.
Crohn’s disease was first described in 1932 by the American physician Burrill Crohn at Mount Sinai Hospital in New York, from whom the condition takes its name.
Crohn’s disease is a chronic, relapsing condition, with most patients experiencing periods of remission interspersed with disease flare-ups. While there is currently no cure, advances in medical therapy over the past decade have significantly improved long-term disease control, quality of life, and reduced the need for surgery in many patients.
The main focus of this article is Crohn disease, but before do this, I give a quick summary of the other main IBD, ulcerative colitis, which has some similarities to Crohn’s, so it important to distinguish between the two conditions.
Ulcerative colitis: A quick overview
Ulcerative colitis (UC) is one of the two principal forms of inflammatory bowel disease (IBD), the other being Crohn’s disease. While both conditions share features of chronic intestinal inflammation, ulcerative colitis has distinct pathological, clinical, and therapeutic characteristics. An understanding of ulcerative colitis is important when discussing Crohn’s disease, as differentiating between the two conditions is central to diagnosis, management, and long-term prognosis.
Ulcerative colitis is a chronic inflammatory condition affecting the colon and rectum, characterised by continuous inflammation of the mucosal lining of the large intestine. Unlike Crohn’s disease, ulcerative colitis does not affect the small intestine (with the exception of limited backwash ileitis in some cases) and does not involve deeper layers of the bowel wall.
The condition typically follows a relapsing–remitting course, with periods of active disease interspersed with remission. Although there is no cure, modern treatment strategies allow many patients to achieve good symptom control and maintain long-term remission.
Causes and pathophysiology
The exact cause of ulcerative colitis remains unknown. It is thought to arise from an inappropriate immune response to intestinal microbiota in genetically sus- ceptible individuals. Environmental factors such as smoking status, infections, diet, and stress may influence disease onset and activity.
In ulcerative colitis, inflammation is confined to the mucosa and submucosa of the colon. This superficial inflammation explains many of the condition’s hallmark symptoms, including bleeding and urgen- cy, and distinguishes UC from Crohn’s dis- ease, where inflammation is transmural.
Clinical features
The most common symptoms of ulcerative colitis include:
- Bloody diarrhoea, often with mucus.
- Urgency and tenesmus (a constant feeling of needing to pass stool). fAbdominal cramping, particularly in the lower abdomen.
- Fatigue, which may be related to inflammation, anaemia, or nutritional deficiency.
Systemic symptoms such as fever and weight loss may occur in more severe disease. As with Crohn’s disease, ulcerative colitis can be associated with extra-intestinal manifestations, affecting the joints, skin, and eyes.
Ulcerative colitis is classified according to the extent of colonic involvement: fProctitis – inflammation limited to the rectum.
- Left-sided colitis – disease extending up to the splenic flexure.
- Extensive colitis (pancolitis) – inflammation involving most or all of the colon.
Disease extent is clinically relevant, influencing symptom severity, treatment choice, and colorectal cancer risk.
Distinguishing ulcerative colitis from Crohn’s disease Although ulcerative colitis (UC) and Crohn’s disease share overlapping features, several key differences help distinguish between them:
- Location: UC affects only the colon and rectum, whereas Crohn’s disease can affect any part of the gastrointestinal tract from mouth to anus.
- Pattern of inflammation: UC causes continuous inflammation, while Crohn’s disease typically produces patchy ‘skip lesions’.
- Depth of inflammation: UC is limited to the mucosal layer; Crohn’s disease is transmural, increasing the risk of stric- tures, fistulas, and abscesses.
- Symptoms: Bloody diarrhoea and urgency are more characteristic of UC, while abdominal pain, weight loss and perianal disease are more common in Crohn’s disease.
- Complications: Crohn’s disease is more likely to cause bowel obstruction, fistulas, and perianal disease; these are rare in UC.
Correct differentiation is essential, as management strategies and surgical ap- proaches differ significantly between the two conditions.
Ulcerative colitis management
Treatment of UC aims to induce and maintain remission, improve quality of life and reduce complications. Options include aminosalicylates, corticosteroids, immunomodulators and biologic therapies, with treatment choice guided by disease severity and extent.
Long-standing extensive ulcerative colitis is associated with an increased risk of colorectal cancer, necessitating regular surveillance colonoscopy.
While ulcerative colitis and Crohn’s dis- ease are closely related, they are distinct clinical entities. The remainder of this ar- ticle will focus specifically on Crohn’s dis- ease in detail, exploring its more complex patterns of involvement, complications, and evolving treatment strategies.
Crohn’s disease
Causes of Crohn’s disease
The exact cause of Crohn’s disease remains unknown. Current understanding suggests it arises from a complex interation of several factors, including:
- Genetic predisposition, with higher risk in first-degree relatives.
- An abnormal immune response to intestinal bacteria.
- Environmental triggers, which may include infections, smoking, diet, stress, and other lifestyle factors.
Research in recent years has increasingly focused on the role of the gut micro-biome, with evidence suggesting altered bacterial diversity may contribute to disease onset and progression. This evolving understanding is beginning to influence future therapeutic strategies.
How Crohn’s disease affects the intestinal tract
Crohn’s disease can affect any part of the gastrointestinal tract, but the most commonly involved area is the terminal ileum, often extending into the first part of the colon near the appendix. In some patients, disease is confined to the colon alone, while others may be involved in multiple, discontinuous sections of bowel, giving rise to the characteristic ‘skip lesions’.
Inflammation may range from a few centimetres to extensive sections of bowel. Because Crohn’s disease often affects the deeper layers of the bowel wall, it is more likely to result in complications. In addi- tion, intestinal inflammation can trigger inflammatory responses elsewhere in the body, leading to extra-intestinal manifestations, commonly affecting the joints, skin, and eyes.
Symptoms of Crohn’s disease
Crohn’s disease is highly variable in its presentation. Symptoms depend on both the severity and location of inflammation and may range from mild to debilitating.
During a flare-up, common symptoms include:
- Abdominal pain and diarrhoea, sometimes containing mucus, pus, or blood.
- Fatigue and tiredness, which may result from inflammation, poor sleep, anaemia, nutritional deficiencies, or weight loss.
- General malaise, occasionally accompanied by fever.
- Mouth ulcers.
- Loss of appetite and unintended weight loss.
- Anaemia, caused by blood loss, reduced dietary intake, or impaired nutrient absorption.
Anaemia remains a major contributor to fatigue in Crohn’s disease and requires active monitoring and management.
Prevalence and risk factors
Crohn’s disease is estimated to affect approximately one-in-650 people in the UK, with prevalence in Ireland thought to be broadly similar. It appears to be slightly more common in women than in men. Irish data indicate ongoing increases in incidence, particularly among younger age groups.
The peak age of onset is between 15 and 35 years, with a smaller second peak later in life. Crohn’s disease diagnosed in childhood often behaves differently and may require a more aggressive treatment approach.
Crohn’s disease is more common in urban populations and in northern, indus- trialised countries. Smoking is a well-established risk factor, associated with both increased disease severity and poorer response to treatment.
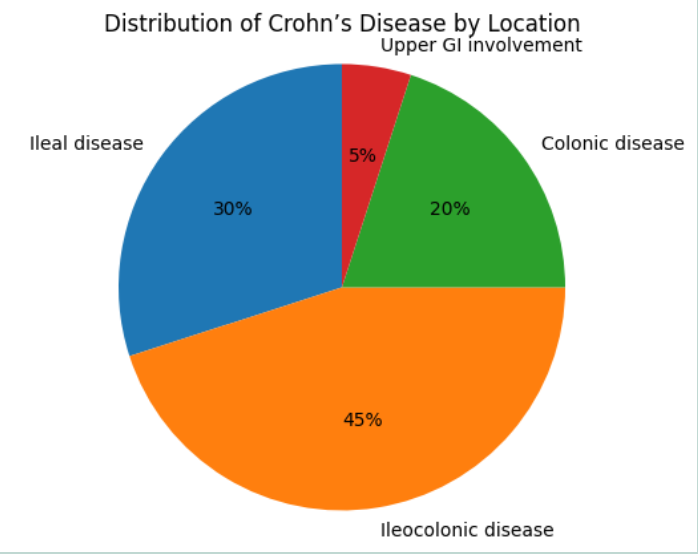
Main types of Crohn’s disease
Terminal iIleal and ileocecal Crohn’s disease
Crohn’s disease affecting the ileum (the final part of the small intestine) is referred to as ileal or terminal ileal Crohn’s dis- ease. When inflammation also involves the beginning of the large intestine, it is described as ileocecal Crohn’s disease.
Patients commonly experience pain in the lower right abdomen, often worsening after meals. Weight loss and diarrhoea are frequent. Because the ileum plays a key role in bile salt absorption, inflammation in this area may result in bile salt malabsorption. Excess bile salts entering the colon can irritate the bowel lining, leading to chronic watery diarrhoea, which is typically non-bloody. Approximately 40 per cent of people with Crohn’s disease have ileal or ileocecal involvement.
Small bowel Crohn’s disease
Crohn’s disease may also affect other parts of the small intestine beyond the terminal ileum. Symptoms are similar to ileal disease and include abdominal pain and diarrhoea, though blood is less com- monly present in stools.
Weight loss, nutritional deficiencies, and anaemia are more prominent features in small bowel disease due to impaired absorption of nutrients. Nearly one-third of patients have Crohn’s dis- ease affecting the small bowel.
Colonic Crohn’s disease (Crohn’s colitis) When Crohn’s disease affects the colon, it is referred to as Crohn’s colitis. This is a common disease pattern and may resem- ble ulcerative colitis clinically.
The predominant symptom is blood-stained diarrhoea, often accompanied by urgency and frequent bowel movements. Inflammation reduces the colon’s ability to store waste, leading to six or more bowel motions per day, particularly when the rectum is involved.
Gastroduodenal Crohn’s disease Crohn’s disease affecting the upper gastrointestinal tract, including the oesophagus, stomach, or duodenum, is relatively uncommon.
Symptoms may include indigestion-like pain, nausea, early satiety, loss of appetite and weight loss. Diagnosis can be challenging, as symptoms may mimic more common upper gastrointestinal conditions.
Perianal Crohn’s disease
Perianal Crohn’s disease affects the area around the anus and may occur alone or alongside intestinal disease. It is associated with significant morbidity and often requires combined medical and surgical management.
Common manifestations include: fAnal fissures, causing pain and bleeding during bowel movements.
- Skin tags, often large and inflamed. fHaemorrhoids, which may be exacerbated by active disease.
- Abscesses, presenting as painful, swollen collections of pus and sometimes associated with fever.
- Fistulas, which are abnormal tunnels connecting the anal canal to surrounding skin or organs.
Perianal fistulas may leak pus or faecal material and can cause considerable discomfort. Management has evolved significantly in the last five-to-10 years, with earlier use of biologic therapy, often in combination with surgery, now recommended for many patients.
Oral Crohn’s disease
Crohn’s disease can occasionally affect the mouth. True oral Crohn’s disease, characterised by swollen lips and deep fissures, is rare. However, mouth ulcers occur in up to one-in-five patients, particularly during periods of active disease.
Complications of Crohn’s disease
Complications may arise within the gastrointestinal tract or affect other parts of the body. Intestinal complications are more common in Crohn’s disease than ulcerative colitis due to the transmural nature of inflammation.
Intestinal complications
Strictures
Chronic inflammation followed by healing can lead to the formation of scar tissue, narrowing the bowel and creating a stricture. This may cause obstructive symptoms such as cramp- ing abdominal pain, bloating, nausea, vomiting and constipation.
Strictures may be inflammatory or fibrotic in nature. While inflammatory strictures may respond to medical therapy, fibrotic strictures often require endoscopic dilation or surgery, commonly in the form of stricturoplasty.
Perforations
In rare cases, severe inflammation or obstruction may cause the bowel wall to rupture, leading to a perforation. This allows bowel contents to leak into surrounding tissues, often resulting in abscess. Perforation is a medical emer- gency requiring urgent intervention.
Fistulas
Fistulas form when inflammation extends through the full thickness of the bowel wall, creating abnormal con- nections between the bowel and other organs, loops of bowel, or the skin.
Management may include antibiotics, immunomodulators, biologic therapies and surgery. In the last few years, anti-TNF agents and newer biologics have become central to fistula management, particularly in perianal disease.
Complications of Crohn’s disease affecting other parts of the body
Crohn’s disease is a systemic inflam- matory condition, and complications are not confined to the gastrointestinal tract. Extra-intestinal manifestations may occur during active disease but can also present independently of bowel symptoms, sometimes preced- ing the diagnosis or persisting during remission.
Joint complications
Inflammatory joint conditions affect up to one-in-three people with IBD. In Crohn’s disease, arthritis is more frequently asso- ciated with colonic involvement.
The most common pattern is peripheral arthritis affecting large joints such as the knees, ankles, wrists, and elbows. Symptoms include pain, stiffness and swelling, often improving as intestinal inflammation is controlled. Long-term joint damage is uncommon in this group.
A smaller proportion of patients develop arthritis affecting the smaller joints of the hands and feet. This form may persist even when bowel disease is in remission.
More rarely, axial arthritis or ankylosing spondylitis may occur, involving the spine and sacroiliac joints. This condition can progress independently of intestinal disease and often requires specialist rheumatology input. Treatment may include biologic therapies, particularly anti-TNF agents, which have shown benefit for both gut and joint disease.
Skin complications
Skin manifestations are relatively common in Crohn’s disease and often parallel disease activity.
Erythema nodosum is the most frequent skin complication, affecting approximately one-in-seven patients. It presents as pain- ful, red nodules, usually on the lower legs, which fade over time leaving bruise-like marks. It typically improves with treatment of underlying intestinal inflammation.
Pyoderma gangrenosum is much rarer but more severe. It begins as small pus- tules or blisters that develop into painful, deep ulcers, most often on the legs or near stomas. Management usually in- volves systemic corticosteroids, immuno- suppressants, or biologic therapies, with increasing use of biologics in refractory cases.
Eye complications
Eye involvement occurs in approximately 5 per cent of patients with Crohn’s disease and should always be treated promptly to prevent long-term damage.
Episcleritis is the most common presentation, causing redness, irritation, and discomfort. It often correlates with bowel disease activity and usually responds to treatment of intestinal inflammation. Uveitis and scleritis are less common but more serious conditions. Symptoms include eye pain, blurred vision, light sensitivity, and headaches. These condi- tions may occur independently of bowel symptoms and often require treatment with topical or systemic steroids, immu- nomodulators or biologic agents.
Patients should be advised to report any new or worsening eye symptoms urgently.
Bone health
People with Crohn’s disease are at increased risk of reduced bone mineral density and osteoporosis. Contributing factors include chronic inflammation, poor calcium and vitamin D absorption, reduced dietary intake and prolonged corticosteroid use.
Assessment of bone health is recommended in at-risk patients, with man- agement including calcium and vitamin D supplementation and, where appropriate, bisphosphonate therapy. Minimising steroid exposure has become a key treatment goal in modern Crohn’s disease management.
Liver and biliary disease
Up to 25 per cent of people with Crohn’s disease develop gallstones, often related to bile salt malabsorption, particularly inileal disease or followingileal resection.
Abnormal liver function tests are relatively common and may be related to fatty liver disease, drug-induced liver injury, or autoimmune conditions.
A rare but important complication is primary sclerosing cholangitis (PSC), which occurs more commonly in patients with colonic involvement. PSC causes inflammation and scarring of the bile ducts and can lead to progressive liver disease. Management is largely support- ive, though ursodeoxycholic acid may be used in selected cases.
Blood clot risk
Crohn’s disease is associated with a two- fold increased risk of venous thromboembolism, including deep vein thrombosis (DVT) and pulmonary embolism. Risk is highest during active disease, hospitalisation, and periods of reduced mobility. Patients should be educated about warning signs such as leg swelling, pain, chest pain, and shortness of breath, and appropriate thromboprophylaxis should be considered during hospital admissions.
Anaemia
Anaemia is a common and often under recognised complication of Crohn’s disease. The most frequent cause is iron deficiency, due to chronic blood loss, reduced intake, or impaired absorption. Anaemia of chronic disease and vitamin deficiencies (particularly vitamin B12 and folate) also occur.
Symptoms include fatigue, breathless- ness, headaches, and reduced exercise tolerance. Management depends on the underlying cause and may include oral or intravenous iron, vitamin supplementation, or treatment of active inflammation. Intravenous iron is increasingly favoured in moderate-to-severe disease due to improved tolerability and efficacy.
Risk of colorectal cancer
Long-standing, extensive Crohn’s disease affecting the colon is associated with a modestly increased risk of colorectal cancer. Risk rises with disease duration, severity, and extent.
Regular surveillance colonoscopy is recommended for patients with colonic involvement, in line with specialist gastroenterology guidance.
Could symptoms be IBS?
Patients with Crohn’s disease may continue to experience bowel symptoms even when inflammatory disease is inac- tive. In such cases, symptoms may be due to irritable bowel syndrome (IBS), which is more common in people with IBD than in the general population.
IBS does not cause intestinal inflamma- tion or bleeding but may result in abdomi- nal pain, bloating and altered bowel habit, including diarrhoea and/or constipation. If investigations show no active inflamma- tion or infection, IBS should be considered. Management may include dietary modification (such as low FODMAP approach- es), stress management and symptom-directed therapy, including peppermint oil or antispasmodics such as mebeverine.
Treatment of Crohn’s disease
Treatment of Crohn’s disease may be medical, surgical, or nutritional, and often involves a combination of approaches. The choice of therapy depends on disease location, severity, complications, and patient factors.
Modern Crohn’s management increasingly follows a treat-to-target approach, aiming not only for symptom control but also for mucosal healing and prevention of long-term complications. There is now greater emphasis on early effective thera- py and minimising corticosteroid exposure.
Drug treatment of Crohn’s disease
The goals of drug therapy are to induce remission during flare-ups and maintain remission long term. Many patients re- quire ongoing treatment for several years.
Anti-inflammatory and immune-modifying drugs Aminosalicylates (5-ASAs)
Drugs such as mesalazine and sulphas- alazine have a limited role in Crohn’s disease and are now used less fre- quently than in the past, as evidence for effectiveness is modest compared with ulcerative colitis.
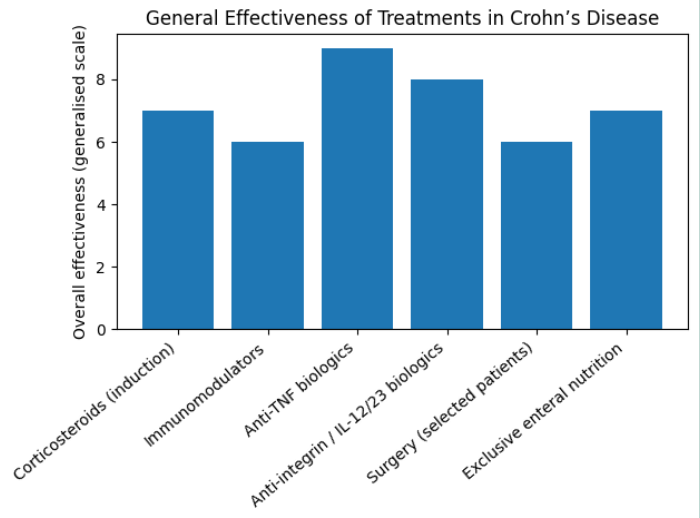
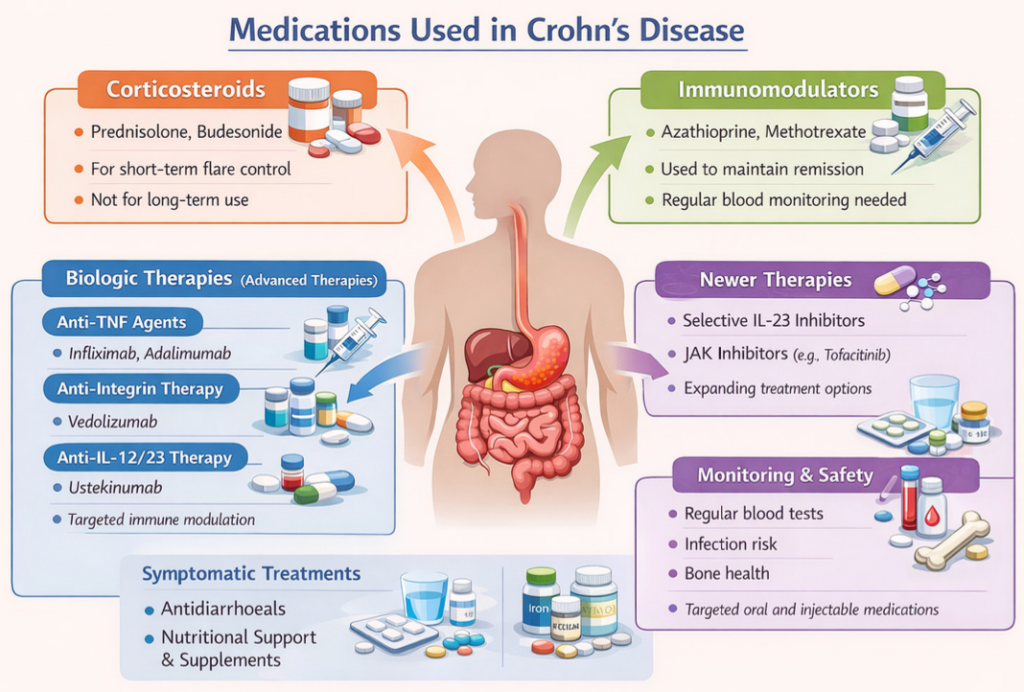
Corticosteroids
Steroids such as prednisolone, hydro-cortisone and budesonide remain effective for short-term control of acute flares but are not suitable for long-term use due to adverse effects. Reducing steroid dependence is now a key objective of Crohn’s management.
Azathioprine, methotrexate and, less commonly, tacrolimus are used to maintain remission or in combina- tion with biologic therapy. Monitoring infection risk, liver toxicity, and blood dyscrasias remains essential.
Biologic and targeted therapies
Over the last five-to-10 years, the use of biologic and targeted therapies has expanded significantly, trans- forming the management of moder- ate-to-severe Crohn’s disease.
Anti-TNF agents
Infliximab and adalimumab remain widely used, particularly in fistulising and perianal disease.
Anti-integrin therapy
Vedolizumab offers a gut-selective mech- anism with a favourable safety profile and is increasingly used in patients with infection risk or comorbidities.
Anti-IL-12/23 therapy
Ustekinumab has become an established option for patients with inadequate response or intolerance to anti-TNF therapy.
Newer agents
More recently, selective IL-23 inhibitors and small-molecule therapies are emerg- ing, further broadening treatment choice and allowing more individualised care. Biologic therapy is increasingly used ear- lier in the disease course for patients with high-risk features. Treatment duration is individualised, with regular reassessment of response and safety.
Symptomatic treatments
Symptomatic treatments may be used alongside disease-modifying therapy to improve quality of life:
- Anti-diarrhoeal agents, such as loper-amide or cholestyramine.
- Bulking agents, such as ispaghula husk.
- Analgesia, with paracetamol preferred; NSAIDs are generally avoided.
Surgical management
Despite advances in medical therapy, surgery remains an important option for Crohn’s disease. It is estimated that up to 70 per cent of patients will require surgery at some stage.
Surgery may be indicated for strictures, fistulas, abscesses, or disease refractory to medical treatment. Current surgical practice favours bowel-preserving techniques, with limited resections and stricturoplasty where possible.
Post-operative recurrence remains common, and early post-surgical medical therapy is now routinely used to reduce relapse risk.
Dietary and nutritional therapy
Enteral nutrition plays an important role, particularly in paediatric Crohn’s disease, where it can induce remission while avoiding steroids. Its role in adults is more limited but may be useful in selected cases or as nutritional support.
There is no single ‘Crohn’s diet’, but maintaining adequate nutrition is essential. Some patients identify dietary triggers, and individualised dietary advice from a dietitian is recommended.
Micronutrient deficiencies, including iron, vitamin B12, folate, calcium and vitamin D, are common and should be actively monitored and corrected. Intra- venous iron and injectable vitamin B12 are often preferred in active disease or malabsorption.
Complementary and alternative therapies
While some patients report benefit from complementary therapies, robust evidence remains limited. Omega-3 supplements, probiotics, and acupunc- ture have not shown consistent benefit in maintaining remission in Crohn’s disease. Patients should be encouraged to discuss alternative therapies with healthcare pro- fessionals to avoid interactions or delayed treatment.
Written by Eamonn Brady MPSI (Pharmacist). Whelehans Pharmacies, 38 Pearse St and Clonmore, Mullingar. Tel 04493 34591 (Pearse St) or 04493 10266 (Clonmore). www.whelehans.ie. Eamonn specialises in the supply of medicines and training needs of nursing homes throughout Ireland. Email info@whelehans.ie
References
1. NICE. Crohn’s disease: management (NG129). National Institute for Health and Care Excellence; 2019 (updated).
2. NICE. Ulcerative colitis: management (NG130). National Institute for Health and Care Excellence; 2019 (updated).
3. Crohn’s & Colitis UK. Crohn’s disease: information and treatment overview; 2023.
4. Crohn’s & Colitis Ireland. IBD facts, figures, and patient resources; 2024.
5. Torres J, et al. Crohn’s disease. The Lancet; 2017.
6. Gomollón F, et al. ECCO Guidelines on therapeutics in Crohn’s disease. Journal of Crohn’s and Colitis; 2020.
7. Feuerstein JD, et al. AGA clinical guidelines for moderate to severe Crohn’s disease. Gastroenterology; 2021.
8. Lichtenstein GR, et al. Management of Crohn’s disease in adults. American Journal of Gastroenterology; 2018.
9. Hanauer SB. Inflammatory bowel disease: epidemiology and pathogenesis. Gastroenterology; 2018.
10. Kaplan GG. The global burden of inflammatory bowel disease. Nature Reviews Gastroenterology & Hepatology; 2015.
11. Peyrin-Biroulet L, et al. Treat-to-target strategies in Crohn’s disease. Clinical Gastroenterology and Hepatology; 2015.
12. Sandborn WJ, et al. Anti-TNF therapy for Crohn’s disease. New England Journal of Medicine; 2012.
13. Feagan BG, et al. Vedolizumab as induction and maintenance therapy for Crohn’s disease. New England Journal of Medicine; 2013.
14. Sandborn WJ, et al. Ustekinumab induction and maintenance therapy for Crohn’s disease. New England Journal of Medicine; 2016.
15. Danese S, et al. Positioning biologics and small molecules in inflammatory bowel disease. Gut; 2020.
16. Sands BE, et al. Management of fistulising Crohn’s disease. Gastroenterology; 2019.
17. Lewis JD. The role of diet and nutrition in Crohn’s disease. Gastroenterology Clinics of North America; 2017.
18. Ruemmele FM, et al. Exclusive enteral nutrition in Crohn’s disease. Journal of Pediatric Gastroenterology and Nutrition; 2014.
19. Gasche C, et al. Anaemia in inflammatory bowel disease. Gut; 2015.
20. Bernstein CN, et al. Extra-intestinal manifestations of inflammatory bowel disease. American Journal of Gastroenterology; 2015.
21. Frolkis AD, et al. Risk of venous thromboembolism in inflammatory bowel disease. Gastroenterology; 2013.
22. Jess T, et al. Risk of colorectal cancer in Crohn’s disease. Gut; 2012






