






Eamonn Brady MPSI reviews the different types of UTI, including gender-specific considerations, self-care, and prevention measures
The urinary tract is responsible for filtering, processing, and excreting liquid waste from the body. Clinically, it is divided into:
- The upper urinary tract: Comprising the kidneys and ureters (which transport urine from the kidneys to the bladder).
- The lower urinary tract: Comprising the bladder and urethra.
Urinary tract infections (UTIs) are classified according to location as either upper or lower UTIs. After respiratory and intra-abdominal infections, UTIs remain one of the most common bacterial infections encountered in clinical practice.
Types of UTI
UTIs are generally classified based on the site of infection:
- Cystitis: Infection of the bladder (lower UTI).
- Urethritis: Infection of the urethra (lower UTI; may also require consideration of sexually-transmitted infections, particularly in younger patients).
- Pyelonephritis: Infection of the kidney (upper UTI).
Classification
UTIs are further categorised as:
Complicated:
Includes infections in men, pregnant women, children, older adults, and those with structural or functional abnormalities, or upper UTIs.
Uncomplicated:
Typically occurs in otherwise healthy, non-pregnant adult women with lower urinary tract symptoms such as dysuria or urinary frequency.
Epidemiology
UTIs are significantly more common in women, with females estimated to be up to 30 times more likely than males to develop an infection. Approximately 50 per cent of women will experience at least one UTI in their lifetime, with many presenting before the age of 25.
Although less common in men (lifetime risk ~10–12%), UTIs in males are more likely to be complicated and may indicate an underlying condition such as prostate disease or urinary obstruction.
In children, UTIs are among the most common bacterial infections, particularly in those under two years of age. Around 8 per cent of girls and 2 per cent of boys will experience a UTI during childhood. Vesicoureteral reflux may be present in a proportion of cases and should be considered in recurrent infections.
In older adults, diagnosis can be more challenging due to atypical presentation. Comorbidities
such as incontinence or cognitive impairment may mask symptoms, and asymptomatic bacteriuria becomes more common with age.
Causes and risk factors
UTIs are most caused by bacteria, typically originating from the gastrointestinal tract, entering the urethra and ascending the urinary tract. In many cases, normal urinary flow helps eliminate bacteria before infection develops.
When host defences are overcome, bacteria may colonise and spread to the bladder or kidneys.
Recognised risk factors include:
- Urinary tract obstruction (eg, kidney stones).
- Sexual activity.
- Diabetes or immunocompromised states.
- Previous history of UTIs.
- Pregnancy.
- Incomplete bladder emptying.
- Catheter use (current or recent).
- Structural abnormalities of the urinary tract.
Gender-specific considerations
Women:
Women are more susceptible due to a shorter urethra and closer anatomical proximity to the rectum, facilitating bacterial entry into the urinary tract.
Pregnancy:
Pregnancy increases UTI risk due to hormonal changes and mechanical pressure on the bladder, leading to incomplete emptying. Screening and treatment are particularly important due to potential complications.
Men:
UTIs are uncommon in younger men but increase with age. Conditions such as benign prostatic hyperplasia (BPH) can impair bladder emptying, increasing infection risk. Prostatitis may also present with UTI-like symptoms and should be considered.
Men who have undergone prostate surgery may also have increased susceptibility due to anatomical changes affecting urinary flow.
Symptoms
Symptoms indicating a lower UTI (cystitis or urethritis) include:
- Increased urination frequency.
- Sudden need to urinate.
- Cloudy or smelly urine (may be indicative of dehydration and not a UTI).
- Burning feeling or pain when passing water.
- Feeling the bladder is not empty after urination.
- General sense of feeling unwell.
- Pain in lower abdomen.
It’s important to note that a lower UTI can quickly develop into something more sinister, so if any of these symptoms persist for more than a few days, or the persons matches any of the statements below, contact the GP.
- Male with UTI symptoms.
- Pregnant with UTI symptoms.
- Blood in urine.
- First time with a UTI.
- Symptoms persist following treatment.
Symptoms of an upper UTI (pyelonephritis) may include in addition to the above:
- Temperature of 38C or above.
Women are more susceptible due to a shorter urethra and closer anatomical proximity to the rectum
- Chills and shivering or shaking.
- Pain in the lower back and/or sides.
- Confusion and agitation (especially in older people).
- Feeling sick or have vomited.
- Diarrhoea.
Generally, someone presenting with any of these symptoms should contact their GP urgently as an undiagnosed kidney infection left untreated can be extremely dangerous.
If the person is very ill, they may need to be referred directly to hospital, especially:
- Elderly people, as there is a much higher risk of sepsis.
- Have cancer, diabetes, MS, or other serious medical conditions that could be compromised by severe infection.
In addition to the above, Children may also:
- Wet the bed – especially in the case of the very young, where they have been consecutively dry for the previous few months; could be a sign of UTI.
- Wet themselves or deliberately avoid urination because it burns or stings.
- With babies, they may be irritable and not feed properly.
Diagnosis
With any of the symptoms above, especially with children or upper UTIs, it is likely that the person will end up at the GP. As with any condition, getting an early diagnosis of the problem will help move quickly to the appropriate treatment and in most cases, if the treatment regimen has been followed, a successful outcome.
The doctor will ask questions to establish the nature and effect of symptoms and traditionally would take a urine sample to test. Urinalysis strips (dipsticks) are the most frequently used method to identify clinical evidence. For most women presenting with ‘typical’ symptoms of a lower UTI, eg, cystitis, urethritis, this test is usually sufficient to confirm a diagnosis and recommend a course of first-line treatment.
As a rule, there are other circumstances where the doctor and recommended diagnostic pathway require the sample to be sent to the lab for further testing, including:
- Any case of UTI in men – this is to rule out other possible causes of symptoms as UTIs in men are relatively rare by comparison.
- Any case where upper UTI is suspected.
- UTI in pregnancy.
- Where there is blood in the urine – again important to assess and rule out other causes eg, bladder cancer.
- Where there is a higher risk factor present due to other conditions that may increase vulnerability to serious complication eg, perhaps a diabetic with a weakened immune system.
There may be other factors where the GP considers further investigation, so other testing methods may be required, such as ultrasound. For example, an ultrasound can help assess early visual condition of kidneys and can also accurately measure ‘before and after’ bladder emptying volume. CT and MRI scans are other diagnostic options. A cystoscopy may also be recommended, where a tiny camera is inserted via the urethra to inspect the bladder, although ironically, this procedure itself carries a risk of UTI.
Treatment
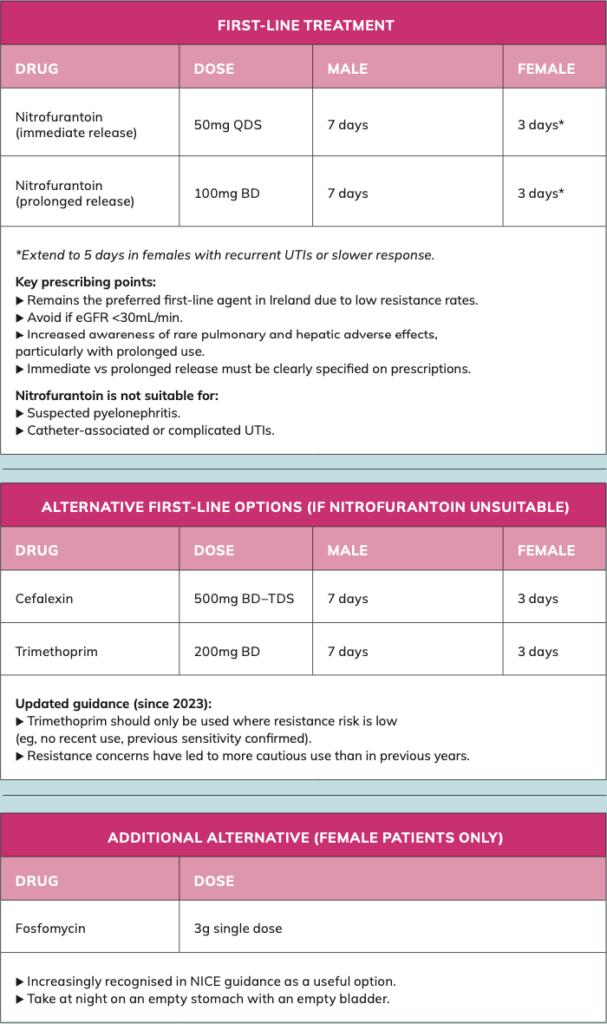
Since I last wrote about UTIs in Irish Pharmacist in 2023, there have been updates in guidance regarding treatment.
Summary of key changes since 2023:
- Introduction of delayed prescribing strategy.
- Stronger antimicrobial stewardship focus.
- More cautious use of trimethoprim.
- Inclusion of methenamine hippurate for prevention.
- Reinforcement of short-course therapy.
- Increased emphasis on non-antibiotic management.
Once a UTI diagnosis is confirmed, management should be individualised based on symptom severity, patient risk factors, and likelihood of complications. While antibiotics remain the mainstay of treatment, there is now a stronger emphasis on antimicrobial stewardship, including the option of delayed prescribing in selected patients.
Patients should be advised to complete the full course of antibiotics if prescribed, even if symptoms improve early, to reduce the risk of relapse and resistance.
In recent years, both HSE and NICE guidance have evolved, with clearer recommendations on first-line choices, treatment duration, and appropriate use of non-antibiotic strategies. Importantly, there is now greater emphasis on avoiding unnecessary antibiotic use in mild cases.
Uncomplicated lower UTIs
General approach
- Consider delayed (back-up) antibiotic prescribing in mild cases:
- Advise use only if symptoms worsen or do not improve within 48 hours.
- Provide symptomatic relief advice:
- Paracetamol or ibuprofen for pain.
- Adequate hydration.
- Exclude red flags (eg, fever, flank pain, pregnancy).
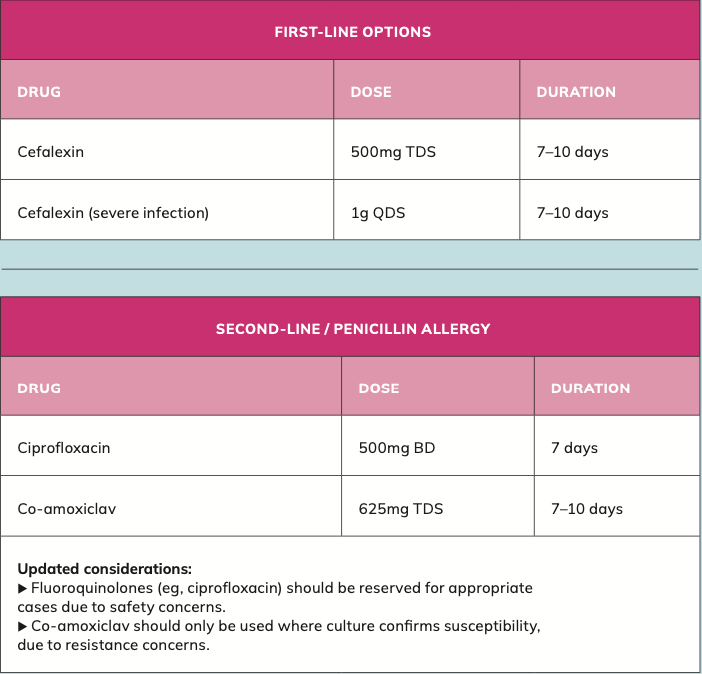
Acute pyelonephritis (kidney infection)
Patients with suspected upper UTI require prompt antibiotic treatment and clinical assessment.
There is now greater emphasis on avoiding unnecessary antibiotic use in mild cases
Prevention and recurrent UTI
Since 2023, there is now significantly greater emphasis on preventing recurrent UTIs and reducing antibiotic exposure.
Non-antibiotic strategies
- Increased fluid intake.
- Post-coital voiding.
- Avoidance of spermicides where relevant.
Utipro Plus AF is an oral capsule option, available without prescription, which can help in the control and prevention of un- complicated UTIs. It acts at an intestinal level to treat UTIs caused by pathogens.
Postmenopausal women
- Topical vaginal oestrogen recommended where appropriate.
Methenamine hippurate
- Now recommended by NICE (2024 update) as a non-antibiotic prophylactic option.
- Suitable for patients with recurrent UTIs where antibiotics are undesirable.
- Works by acidifying urine and preventing bacterial growth.
Key stewardship messages
- Avoid treating asymptomatic bacteriuria (except in pregnancy).
- Use shortest effective antibiotic course.
- Consider delayed prescribing where appropriate.
- Review recurrent cases carefully before initiating long-term antibiotics.
Self-care and prevention
When offering advice on how patients can help themselves prevent UTIs, consider the following practical measures:
Do
- Toilet hygiene – wipe from front-to- back to reduce transfer of bacteria towards the urethra.
- Fully empty the bladder when urinating – reduces urinary stasis and infection risk.
- Maintain good fluid intake – helps flush bacteria from the urinary tract.
- Shower instead of prolonged baths, particularly if prone to recurrent UTIs.
- Wear breathable underwear (eg, cotton) and avoid overly tight clothing.
- Urinate as soon as possible after sexual intercourse.
- Maintain a regular but gentle genital hygiene routine.
Do not
- Use perfumed soaps, bubble baths, and intimate hygiene products, which may irritate the urethra.
- Do not delay urination – regular bladder emptying is important.
- Avoid spermicidal contraceptive products, which are associated with increased UTI risk.
Natural options
- Cranberry products: Evidence remains mixed; not routinely recommended.
- Probiotics and yoghurt: Insufficient evidence to support routine use.
- Methenamine hippurate: Recognised as a non-antibiotic preventive option for recurrent UTIs.
- Topical vaginal oestrogen: Recommended for postmenopausal women with recurrent UTIs.
Advice to patients
UTIs are very common, particularly in women, and in many cases are mild and self-limiting. There is now a greater emphasis on managing symptoms conservatively where appropriate. These can often be managed initially with:
- Paracetamol or ibuprofen for pain.
- Adequate hydration.
Some patients may be suitable for a delayed antibiotic approach, where treatment is only started if symptoms do not improve or worsen within 48 hours. Patients should seek medical review if:
- Symptoms persist beyond 48 hours.
- Symptoms worsen rapidly.
- Fever, flank pain, or systemic symptoms.
- They are pregnant, male, or have recurrent UTIs.
Author: Eamonn Brady MPSI (Pharmacist). Whelehans Pharmacies, 38 Pearse St and Clonmore, Mullingar. Tel 04493 34591 (Pearse St) or 04493 10266 (Clonmore). www.whelehans.ie Eamonn specialises in the supply of medicines and training needs of nursing homes throughout Ireland. Email info@whelehans.ie
References
• Health Service Executive (HSE) (2026) Uncomplicated UTI in adult non-pregnant females (V2.2). Dublin: HSE. Available at: https:// healthservice.hse.ie.
• Health Service Executive (HSE) (2023) Common Conditions Service Protocol: Uncomplicated Lower Urinary Tract Infection. Dublin: HSE. Available at: https:// healthservice.hse.ie.
• Health Service Executive (HSE) (2024) Antimicrobial Resistance and Infection Control Programme (AMRIC): Guidelines. Dublin: HSE. Available at: https://healthservice. hse.ie.
• Health Service Executive (HSE) (2025) Antimicrobial Prescribing Guidelines for Primary Care. Dublin: HSE. Available at: https:// healthservice.hse.ie.
• Medical Independent (2024) Treating urinary tract infections. Dublin: GreenCross Publishing. Available at: https://www.medicalindependent.ie.
• Health Protection Surveillance Centre (HPSC) (2023) Antimicrobial resistance in Ireland report. Dublin: HPSC. Available at: https://www.hpsc.ie.
• Irish College of General Practitioners (ICGP) (2023) Management of urinary tract infections in primary care. Dublin: ICGP. Available at: https://www. icgp.ie.
• Pharmaceutical Society of Ireland (PSI) (2024) Guidance for pharmacists on antimicrobial stewardship. Dublin: PSI. Available at: https://www.psi.ie.
• Health Service Executive (HSE) (2023) Urinary tract infection guidance for children. Dublin: HSE. Available at: https://healthservice. hse.ie.
• Health Service Executive (HSE) (2025) Adult antimicrobial prescribing guidance summary. Dublin: HSE. Available at: https:// healthservice.hse.ie.
• National Institute for Health and Care Excellence (NICE) (2023) Urinary tract infection (lower): antimicrobial prescribing (NG109). London: NICE. Available at: https://www.nice.org.uk.
• National Institute for Health and Care Excellence (NICE) (2023) Urinary tract infections in adults: Quality Standard (QS90). London: NICE. Available at: https://www. nice.org.uk.
• National Institute for Health and Care Excellence (NICE) (2024) Recurrent urinary tract infection (NG112). London: NICE. Available at: https://www.nice.org.uk.
• National Institute for Health and Care Excellence (NICE) (2023) Antimicrobial stewardship. London: NICE. Available at: https://www.nice.org.uk.
• UK Health Security Agency (UKHSA) (2023) Diagnosis of urinary tract infections: quick reference tool. London: UKHSA. Available at: https://www.gov.uk.
• European Association of Urology (EAU) (2024) Guidelines on urological infections. Arnhem: EAU. Available at: https://uroweb.org.
• Gupta, K. et al. (2023) International clinical practice guidelines for acute uncomplicated cystitis and pyelonephritis. Clinical Infectious Diseases. Available at: https://academic.oup.com.
• Flores-Mireles, AL et al (2022). Urinary tract infections: epidemiology, mechanisms and treatment options. Nature Reviews Microbiology. Available at: https:// www.nature.com.
• World Health Organisation (WHO) (2023) Antimicrobial resistance and stewardship guidance. Geneva: WHO. Available at: https://www.who.int.
• National Centre for Biotechnology Information (NCBI) (2024) Urinary tract infections
in adults – clinical overview. Bethesda: NIH. Available at: https://www.ncbi.nlm.nih.gov.






