In summer 2023, ‘business’ at vaccination centres was at very low levels. During this time, the pharmacy staff (one pharmacist (me) and one pharmacy technician) in South East Community Healthcare (SECH) and Suicide Prevention Officers agreed a collaboration to run a DUMP campaign across the five counties of the region — Carlow, Kilkenny, South Tipperary, Waterford, and Wexford.
The Vision of Connecting for Life (CfL) is: ‘An Ireland where fewer lives are lost to suicide.’ All actions in the Strategy relate to seven over-arching goals, and Goal 6 is ‘to reduce and restrict access to means of suicidal behaviour’. The development and delivery of DUMP campaigns at local, regional and national level aligns with Goal 6.
The campaign also aligns with the pillars of the National Drug Strategy: Reducing Harm, and Supporting Recovery 2017-2025. Both strategies were developed using an international body of evidence for suicide prevention and harm reduction.
Pilot campaign
The campaign in SECH began with an initial meeting between the Vaccination Service Pharmacist and the Suicide Resource Office Team, where it was agreed to do a pilot DUMP Campaign in Waterford for the month of May. When the vaccination bases were open to the public, the DUMP facility was available at the same time.
Members of the public could bring any unwanted medication to the centre, where a member of the pharmacy staff met them and took their bags/boxes from them, while also offering information and advice if required. The Waterford Centre yielded promising results and a decision was made to extend the Campaign to the other four counties in SECH, (Carlow, Kilkenny, South Tipperary and Wexford), for the months of July and August.
Communication
The HSE Regional Suicide Resource Office and the Vaccination Service worked with HSE Communications to develop press releases, articles, posters and informational materials for the campaign. Campaign promotional literature was distributed to all Connecting for Life Partners in SECH, to the GPs and to the pharmacies throughout the region. This happened via email and mail drop.
The campaign was advertised on local media, and I did a number of interviews on local radio that increased interest in the campaign. Promotional materials were visible at the Vaccination Centres.
Over the four-month period, approximately 500kg of medication was collected across the five counties
Disposal
A specialist Medicine Disposal Company was engaged to dispose the medicines received in a safe and environmentally appropriate manner. The company provided 60-litre bins for the returned medication — aerosol products had to be segregated and disposed of in separate bins and every effort was made to recycle as much packaging as possible.
All packaging was removed, all tablets were removed from blister packs, and identifying labels were destroyed. All data collected was anonymised. Each time a bag/box of medication was received, it was given a lot number, and this matches the number of people who came to dispose of medication. This also allowed for comparisons between the counties. All medicines were opened, identified, counted and documented manually.
A spreadsheet was populated to collate all the information. While this process was quite laborious, it was an effective way to capture the types and quantities of unused medications that are in people homes. ‘Sharps’ (used needles/ lancets) were not accepted, — anyone presenting with these items was directed to the appropriate HSE sharps collection point. Veterinary medicines are not included in this report, although a small amount was received.
Over the four-month period, approximately 500kg of medication was collected across the five counties. The most commonly returned drug was paracetamol or paracetamol-containing products, and as previously stated, paracetamol is one of the most commonly-used drugs in intentional overdoses.
Results:
- 390 people returned bags/boxes/vanloads(!) of medications.
- There were 6,908 individual items within these bags.
- In total, 305,612 individual tablets/capsules, etc, were de-blistered and placed in disposal buckets.
- Most items were identifiable by the pharmacist, and less than 10 per cent were not identifiable (see below).
| Carlow | Wexford | Waterford | Kilkenny | South Tipperary | Total | |
| Number of clinic days | 4 | 9 | 5 | 5 | 4 | 27 |
| Number of lots collected | 71 | 118 | 69 | 64 | 68 | 390 |
| Average lot per clinic day | 18 | 13 | 14 | 13 | 17 | 15 |
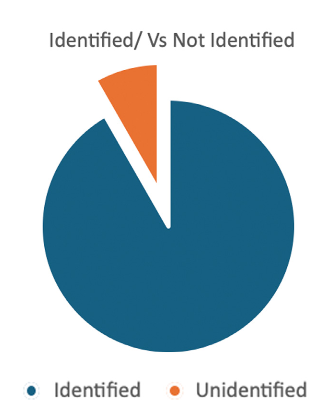
| Identified medicines (number of tablets/ capsules) | 277,555 |
| Unidentified medicines | 25,057 |
- 22 x 60-litre buckets with loose powder, liquids, tablets and capsules, and another 60-litre container of aerosols.
- Disposed of 130 white sacks full of packaging — boxes, blister packs, tablet containers for recycling.
- Washed, sterilised, and recycled 550 glass containers.
- There were approx 48kg of powders, creams, sachets, ointments.
- There were approx 72 litres of oral medication — cough bottles, lotions, etc.
Please note: Weights and volumes are not measured, guesstimate based on pack size and how much remained in the tube/bottle.
Number of items per lot
| Carlow | Wexford | Waterford | Kilkenny | Sth Tipperary | |
| Smallest no of items | 2 | 3 | 2 | 2 | 3 |
| Largest no of items | 80 | 60 | 50 | 65 | 89 |
| Total items returned | 1,192 | 2,252 | 948 | 1,005 | 1,511 |
| Average number of items per lot | 17 | 19 | 14 | 16 | 22 |
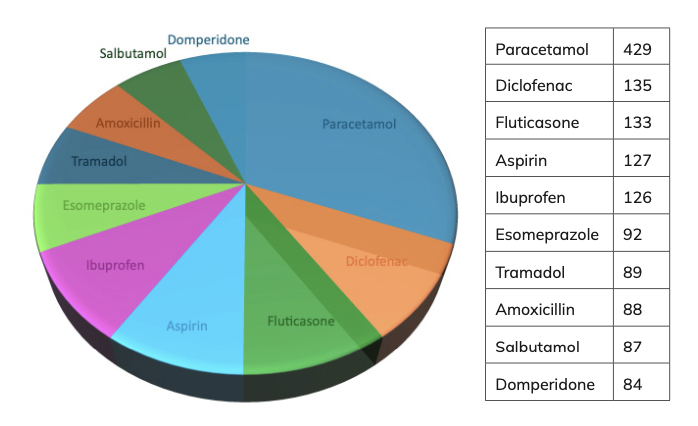
The chart below shows the 10 most commonly returned items, listed with the number of different lots they were returned in.
| Paracetamol | 429 |
| Diclofenac | 135 |
| Fluticasone | 133 |
| Aspirin | 127 |
| Ibuprofen | 126 |
| Esomeprazole | 92 |
| Tramadol | 89 |
| Amoxicillin | 88 |
| Salbutamol | 87 |
| Domperidone | 84 |
Paracetamol or paracetamol-containing products were the most commonly returned item. This is concerning, as it is one of the most commonly used drugs in intentional overdose.
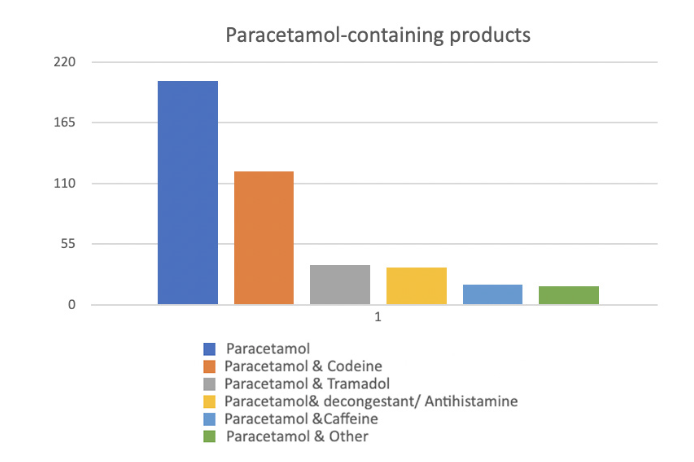
The breakdown in paracetamol-containing products is shown below with the number of lots that had such a product.
| Paracetamol | 203 |
| Paracetamol & codeine | 121 |
| Paracetamol & tramadol | 36 |
| Paracetamol & decongestant/antihistamine | 34 |
| Paracetamol & caffeine | 18 |
| Paracetamol & other | 17 |
Evidence of non-compliance with prescribed medication
The most commonly returned items that showed non-compliance are from the following categories of drugs:
- Respiratory – inhalers and nebules.
- Diabetes – Testing strips/lancets/needles.
- Nasal sprays.
- Eye drops and ointments.
- Topical creams.
- Vitamin and minerals.
There were over 100 items where more than a year’s supply was returned from one household. Much of this medication was in sealed packs, and in date.
This included: 2,514 Artelac SDU (3.5 years’ supply), 48 Dymista Nasal Spray (4 years’ supply), 59 tubes of Hylo Night eye ointment (five years’ supply), 1,587 Onbreez Capsules for inhalation (4.4 years’ supply), 89 Beclazone Evohalers (over 6 years’ supply).
Interesting facts
Throughout the course of the DUMP Campaign, some interesting facts emerged:
- The oldest medication returned was from 1963.
- Many bags/boxes returned had multiple versions of the same drug, ie, four types of Aspirin (Nuprin, Nuseals Aspirin, Aspirin Krka and Disprin).
- There were multiple occurrences of generic and branded medicines in the same lot, ie, Exforge and Valsartan/Amlodipine, Nexium and Esomeprazole.
- In many bags/boxes returned, there was some duplication of prescription items containing the same ingredients as over-the-counter products.
- Some products are very difficult to get out of their packaging, an observation here is that this could cause problems for those using the medication.
- 10 people returned the Government-supplied iodine tablets (126 tablets) from circa 2002.
- There were thousands of capsules with powder for inhalation returned without the inhaler device, ie, Spiriva/Onbreez. This could suggest that those prescribed may not know how to use the product.
- There were 76 Paxlovid tablets returned; this is a very expensive treatment for Covid-19 on the specialist prescribing list, and this included two untouched treatment courses.
- One person found a black sack of tablets in the attic of a recently purchased house that contained the medication of a former resident. It appeared that the medicines were collected every month for three years — all bags remained sealed by the pharmacy label and not one tablet was taken.
- Many people returned medication from a deceased family member and explained that they couldn’t bring themselves to dispose of it earlier.
- One person returned fertility drugs that they had for 10 years.
- Veterinary returns included a calf drench, dog and cat powders and wormers. These were not documented; one client returned 15kg of veterinary medicines.
- Numerous people came with medication and went on to get the Covid booster vaccine while they were at the centre.
- Several people commented on having heard about the campaign on local radio, which prompted them to use the service. Local radio was the publicity that was most commented on.
- Everyone who availed of the service was very appreciative and complimentary and it was noted by many that this service should be provided nationwide and repeated regularly.
In our Mini Dump Campaign in SECH last summer, 390 homes took park. These 390 homes generated €107,748.88 in wasted medication
The financials
The method used to establish the cost of each item is as follows:
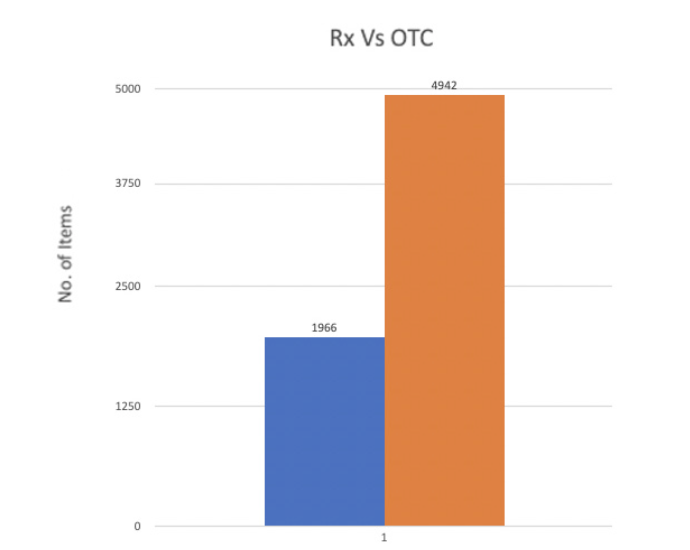
1. Only prescribed medication are included. All OTC and unidentified products were excluded.
2. Prices are from PCRS list effective April 24 2024.
3. Unlicensed medications are not included.
4. All medication is priced as the cheapest generic brand. For example, Lyrica was priced as Pregabalin, etc.
In our Mini Dump Campaign in SECH last summer, 390 homes took park. These 390 homes generated €107,748.88 wasted medication.
The high-tech meds and Paxlovid returned were valued at €15,273.79
Three-hundred and ninety homes represent 0.02% of all occupied homes. (From 2022 Census, there are 2,124,590 permanent dwellings in Republic of Ireland (66,752 of these are vacant), so the occupied housing is 1,858,526.)
Some of the returned medication was part packs, medication not finished, or changed. From the Primary Care Reimbursement perspective, this waste may be reduced, but could never be eliminated completely. So, to evaluate this waste in terms of excess medication and the potential to reduce this waste in the future, I excluded all items where there was less than three months’ supply returned. This will give a more realistic figure for medication waste that could potentially not be dispensed/prescribed.
This was calculated using the permitted maximum dose for each drug. For example, 8 paracetamol 500mg is the maximum daily dose, that is 240 per month, or 720 for three months’ supply. For example, in this exercise, any paracetamol returned in a quantity of less than 720 was excluded.
Using these criteria, the cost price of the medication returned was €54,956.
Waste
Using these figures as a guide to potential waste across the country, 0.02% of homes provided €54,956 unnecessary medication waste.
If that figure is extrapolated:
- If 1% of homes have this waste, that is costing the State €2,747,800.
- If 10% of homes have this waste, that is costing the State €27,478,000.
- If 20% of homes have this waste, that is costing the State €54,956,000.
- If 30% of homes have this waste, that is costing the State €82,434,000.
- If 40% of homes have this waste, that is costing the State €109,912,000.
The breakdown of excessive waste by drug category is broken down in the following graphic.
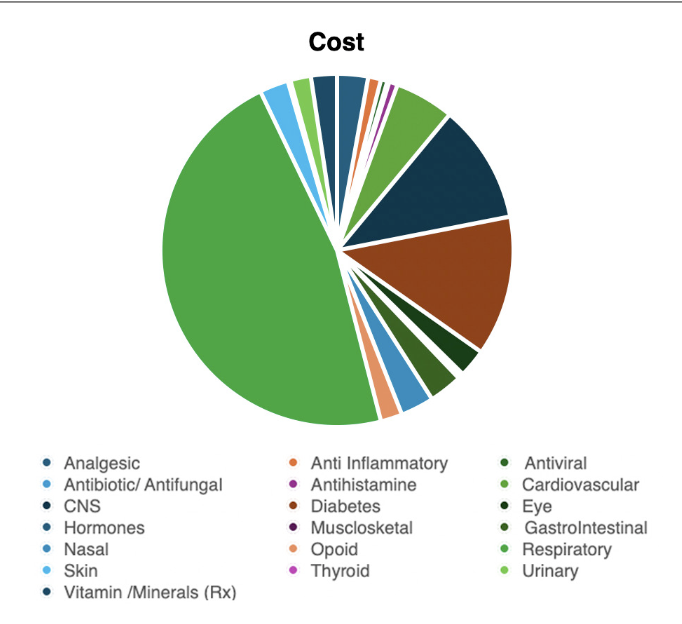
| Cost | % of total | No of times in excess of 3 months supply was returned | |
| Analgesic | €1,536.33 | 2.80 | 20 |
| Anti Inflammatory | €635.47 | 1.16 | 11 |
| Antiviral | €322.8 | 0.59 | 3 |
| Antibiotic/ Antifungal | €96.04 | 0.17 | 5 |
| Antihistamine | 425.64 | 0.77 | 4 |
| Cardiovascular | €2,939.97 | 5.35 | 93 |
| CNS | €5,897.84 | 10.73 | 44 |
| Diabetes | €6,944.46 | 12.64 | 50 |
| Eye | €1,401.87 | 2.55 | 18 |
| Hormones | €82.27 | 0.15 | 3 |
| Musculoskeletal | €196.46 | 0.36 | 30 |
| Gastrointestinal | €1,656.13 | 3.01 | 40 |
| Nasal | €1,654.53 | 3.01 | 53 |
| Opoid | €1,073.9 | 1.95 | 4 |
| Respiratory | €25,331.09 | 46.09 | 104 |
| Skin | €1,428.3 | 2.60 | 12 |
| Thyroid | €136.05 | 0.25 | 14 |
| Urinary | €1,016.81 | 1.85 | 8 |
| Vitamins/minerals (Rx) | €1,288.86 | 2.35 | 29 |
In terms of the cost of wasted medication, Respiratory drugs (inhalers/nebules) are most expensive, followed by diabetic drugs and associated equipment (lancets, needles, strips), and then central nervous system drugs.
In terms of the number of times each class of drug was returned with a quantity in excess of three months, respiratory drugs are again top of the list, followed by cardiovascular drugs, and then nasal medication.
This accumulation of medication poses a risk for those vulnerable
to suicide and self- harm, as it increases access to means
Apart from the financials, there are serious issues around patient compliance evident in this study, and that being the case, there is likely extra hospital days/treatments and possible deaths because medication was not taken as prescribed.
Conclusions
There are considerable quantities of medication in homes throughout Ireland and there appears to be a lack of information for the public on how to dispose of medicines safely. This accumulation of medication poses a risk for those vulnerable to suicide and self-harm, as it increases access to means.
For the State, there is a significant cost associated with unused and unwanted medication in terms of funding for treatment and for patients who are paying for prescriptions that are not being used. A large quantity of OTC medication, purchased by the general population, was also returned, and this is an additional cost for the end user.
Many of those presenting to the DUMP sites stated that they felt unable to explain to the GP or pharmacist that they had an adequate supply and did not need all items refilled every month. Some also reported that they did not necessarily understand how to take the medication if a prescription changed or increased.
Medications that were prescribed for use ‘as needed’ seemed to accumulate more than others, ie, inhalers, eye drops, constipation treatments, etc. Medication storage within homes is sometimes far from ideal, as many of the products returned were damp, mouldy, dirty, showed evidence of rodents, or were well past their expiry dates. The DUMP Campaign in SECH was fruitful and was an innovative way of collaborating and sharing resources.
Recommendations
· A national population-based DUMP campaign should be considered to reduce the amount of medicines that people have in their homes, this report gives an indication of how vast that amount may be, this should be rolled-out with input from all relevant stakeholders, including GPs, pharmacists, mental health and substance misuse services, the Environmental Protection Agency, etc.
· The benefits in SECH included the expertise of the community pharmacist and the ability of the HSE Resource Office to promote the campaign by reaching into communities and by using existing stakeholder relationships to promote the campaign.
· Any such campaign should have a comprehensive, far-reaching communications plan so that all demographic groups are informed.
· Different DUMP sites should be considered to accommodate as many people as possible, ease of access and stigma reduction should be taken into account, ie, GP surgeries, health centres, pharmacies, public venues, mental health and substance misuse centres, etc.
· Further engagement and medication management between the patient and their GP should be explored, ie, does the patient need medication this month or is there some at home? This is especially important for bulk items or ‘as needed’ items, ie, testing strips, lancets, needles, paracetamol, nebules, inhalers, sachets, etc.
· Pharmacy staff could also engage with the patient before dispensing a prescription to check if every item is needed, ie, if a patient uses one injection a day, then the box containing 200 needles is only needed every six months and should not be dispensed more often than this.
· There could be further checks placed on Government Contract Schemes, ie, GMS, LTI, DPS, EU, HAA, High-Tech, etc, where the patient is given an opportunity to state whether they need every medication or not.
· Patients need to be able to explain to their GP or Pharmacist why they are not taking a prescribed medicine or if they have enough at home.
· The process for disposing of veterinary medicines is unclear; this warrants further exploration and communication to relevant agencies. Equally, information on the disposal of sharps should be given at the campaign communication stage.
· Funding for DUMP campaigns nationally should be multi-sectoral to include all relevant stakeholders. The financial evaluation proves there is plenty of scope to pay for this service out of savings that would be generated to the PCRS.
· It is worth considering embedding a research/evaluation component into any further campaigns, as there is little evidence available to support the effectiveness of such a campaign in reducing self-harm or suicidal behaviour.
Recommendations for further education, information and awareness
For prescribers/pharmacists:
- Is the prescription due?
- Is it required?
- Is the patient getting large quantities of PRN items, are they needed?
- Is the requested quantity reasonable and consistent with best practice?
- For new items, small quantities should be prescribed to establish tolerance and efficacy.
For the patient:
- How do I take/use my medication?
- Is it important to take it the entire time/when can I stop?
- How do I store my medication?
- How do I dispose of excess medication?
- Why is it is important not to take medication from the pharmacy that I do not need or that I already have at home?
- Do I have multiple versions of the same drug?
- What are the dangers of accumulating medications in my home for me and/or for others around me?
For medical product manufacturers:
- Are the instructions for use clear and easily understood?
- Can there be a larger print for expiry dates?
- Are there clear directions on how to dispose of each component of the product?
For the Dept of Health/PCRS
- Please do something about this waste of taxpayers’ money!
Fiona Maher qualified from Trinity College Dublin in 1990 and worked in community pharmacy in Waterford city from 1990 until 2021.
Fiona was the pharmacist for the mass vaccination centre in Waterford and that role evolved to be the South East Community Healthcare Vaccination Pharmacist, as well as being Vice Chair of the National Covid vaccine stewardship group. Fiona has now taken up a role in Ayrfield Medical Practice in Kilkenny, working as a pharmacist for prescription review/ reconciliation in a busy general practice.