Dr Donna Cosgrove MPSI provides an overview of treating tiredness and fatigue
Fatigue refers to a set of subjective symptoms that can include tiredness, weakness, lack of energy, and inability to concentrate.3 It can be a normal response to daily life that disappears after resting; however, chronic or uncontrolled fatigue which is not relieved with rest are medical issues that impair productivity and reduce quality of life.
Physical fatigue is a form of tiredness due to repeated muscle movements. This is distinct from mental fatigue, which is defined as “a psychobiological state of tiredness caused by prolonged periods of performing demanding, cognitive-load-inducing activities”.2 Stress is distinct from mental fatigue, although the two frequently coexist. Stressors result in the release of hormones like cortisol and adrenaline, which lead to behavioural and physical changes (‘fight or flight’), rather than a feeling of tiredness and depletion.
Mental fatigue is characterised primarily by tiredness, reduced alertness, and impaired cognitive performance, whereas stress is associated with physiological arousal and emotional responses such as anxiety, frustration or panic. If stress is long term, however, this can disrupt normal cognitive functions, sleep, and digestion, and be a cause of mental fatigue.
Fatigue is among the most common reasons for people presenting in primary care, and is prevalent bothin people who have been diagnosed with medical conditions, and in those without any specific diagnosis.1 It
is particularly common in cancer, affecting approximately half of patients, and substantially more during active treatment. Because fatigue is such a non-specific symptom appearing in many types of diseases, differentiating between primary, secondary or comorbid fatigue can be challenging. Unexplained fatigue is three times more common than explained fatigue, which has a clear identifiable cause (physical, mixed, mental or drug induced). Unexplained fatigue is more difficult to manage, and often associated with a lower quality of life.
Clinically, fatigue is classified by duration, severity, or the existence of an underlying condition. Chronic fatigue (?6 months) commonly presents as severe fatigue leading to significant impact on daily life, including poor mental health. A systematic review1 estimated the prevalence of chronic fatigue to be about 8 per cent, with general fatigue (<6 months) having an average prevalence of 24 per cent in adults.
Causes of tiredness and fatigue
Fatigue is often multifactorial rather than attributable to a single deficiency.3 Causes of mental fatigue include high-pressure occupations, long working hours, poverty, and long periods of activities that require high levels of executive functioning (working memory, attention, flexible thinking, self-control). Work-life balance is important — it has been shown that longer working hours increase general fatigue, physical disorders, anxiety, and chronic tiredness.2 Tiredness is usually self-limiting and explained
by obvious causes, but sometimes fatigue itself may be indicative of disease development. Potential contributing factors such as anaemia, hypothyroidism, mental health conditions, or ME/CFS may need to be investigated and addressed.1,3
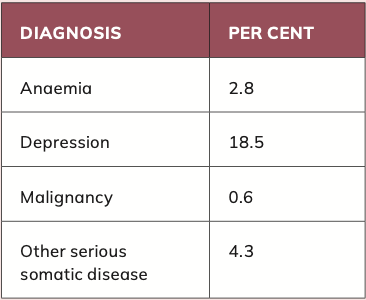
On one hand, an observational study1 found that 47 per cent of adults with a new episode of fatigue received one or more medical diagnoses in the following year, including infections, anaemia, thyroid dysfunction, diabetes, and cancer. However, on the other hand, a systematic review/meta- analysis of 26 studies3 investigating the differential diagnoses of tiredness among individuals presenting to their GP found serious somatic disease to be rare. Table 1 shows the most common diagnoses.
Although anaemia, malignancies and other somatic diseases were found to be rare in this study, it is notable that nearly one-in-five people presenting with tiredness was identified as having a depressive disorder.
Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) is a poorly-defined condition. The terms ME, CFS and ME/CFS are often used interchangeably, although evidence of brain inflammation is limited. No definitive diagnostic test exists. The underlying cause remains unclear, but symptoms are frequently triggered by infection. According to NICE guidance,4 ME/CFS is suspected if the following symptoms have been present for a minimum of six weeks:
- Debilitating fatigue that is worsened by activity, not caused by any excessive
Fatigue is often multifactorial rather than attributable to a single deficiency
exertion, and not relieved by rest.
- Post-exertional malaise after activity with symptoms that are often delayed in onset by hours or days, disproportionate to the activity, and prolonged recovery time.
- Unrefreshing sleep or sleep disturbance.
- Cognitive difficulties, often described as ‘brain fog’, such as problems finding words or numbers, difficulty speaking, slowed responsiveness, short-term memory issues, difficult concentrating or multi-tasking.
ME/CFS is a fluctuating condition with variable symptoms and long-term outcomes. No medicines or supplements have been shown to cure ME/CFS, but supportive care including adequate hydration, a balanced diet, management of comorbidities, and, where appropriate, CBT as an addition to symptom management, is recommended.
Medications and fatigue
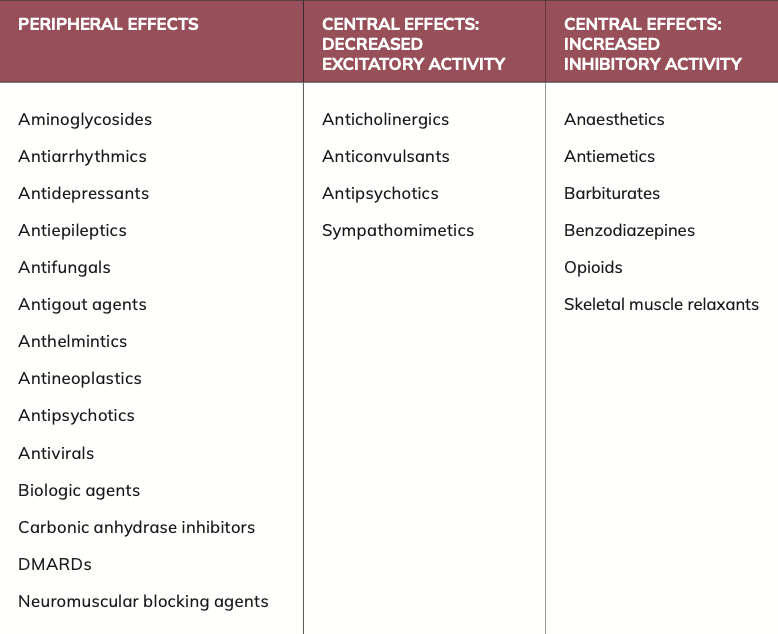
One of the most common adverse effects of medication is fatigue.5 Cholinergic and muscarinic agonists cause increased arousal, therefore it makes sense that antagonists have the opposite effect, potentially leading to fatigue. Some antimuscarinics (eg, scopolamine, oxybutynin) can cause central adverse effects, including drowsiness and cognitive impairment. Other drugs like first-generation antihistamines (eg, diphenhydramine) have anticholinergic properties that cause CNS depression. This is much
less prominent in second-generation antihistamines, although fatigue and somnolence are still commonly reported.
Sympathomimetics (adrenergic receptor agonists/antagonists) also affect excitatory CNS activity. Most drugs in this class act peripherally, with the exception of the alpha 2 adrenergic agonist clonidine, which is used to treat multiple conditions, including hypertension. Beta blockers, although believed to exert their activity peripherally, nonetheless cause fatigue in a minority of patients.
In some conditions, including epilepsy, reduced CNS activity is the desired treatment effect. Drugs used in epilepsy reduce the release of excitatory neurotransmitters in the brain through different mechanisms: Sodium channel blockade (phenytoin, carbamazepine), decreasing low threshold calcium currents in the CNS (ethosuximide), a combination of these (valproic acid), or binding to presynaptic vesicle protein 2A (levetiracetam).
In other clinical conditions like pain or anxiety, increasing the inhibitory activity of the CNS can be desirable. Barbiturates and benzodiazepines enhance the inhibitory effects of GABA, and baclofen acts as an agonist on the GABA B receptor subtype, commonly leading to drowsiness and fatigue as side-effects. Opioids act primarily on mu and kappa opioid receptors in the CNS, altering pain perception, but also causing sedation.
Another contributing factor to fatigue is reduced oxygen-carrying capacity in the body. There are multiple pathways in this process that can be affected by drugs, of which the most common is interruption of haematopoiesis (the formation of blood cellular components). Drug classes that can impact this include antineoplastics, certain anti- infective agents (ie, antiparasitic
In other clinical conditions like pain or anxiety, increasing the inhibitory activity of the CNS can be desirable
agents, antivirals, antiretrovirals, and antifungals), antipsychotics, antidepressants, anticonvulsants, drugs used in the treatment of rheumatoid arthritis, and certain biologic agents.
For many drugs, the mechanism behind the cause of fatigue is unknown: Even placebo treatments can cause fatigue in patients.
Supplements for fatigue
There is a strong biological and physiological basis to indicate that the involvement of certain vitamins and minerals in energy production translates into functional and physiological outcomes, such as perceived fatigue (both physical and mental), and psychological and cognitive functions.6 Although severe deficiency states are relatively uncommon in developed countries, suboptimal micronutrient status remains common and may contribute to fatigue in susceptible individuals. Both food choices and the types of food available can contribute to this.
- All of the B vitamins (except folate) are involved in biochemical energy production systems in the cell.
- Vitamin C is needed for the synthesis of carnitine, which transports fatty acids into the mitochondria, ultimately producing ATP for energy release.
- Iron is included in cytochromes, a type of protein that acts as vital electron carriers within cells needed for energy production.
- Magnesium is important for the production and use of ATP.
There is a close interplay between these micronutrients in the process
Iron and B vitamins are also important for erythropoiesis, red blood cell generation
of energy production, so it is important that they are all available simultaneously — the process can be slowed down by a deficiency in any one of them. In addition to energy production, oxygen delivery from erythrocytes to, eg, the brain and muscles, is needed. Iron and B vitamins are also important for erythropoiesis, red blood cell generation. Vitamin C is important to deal with reactive oxygen species generated from respiration.
The importance of sleep
Sleep is fundamental for multiple biological functions in our bodies. The impact of impaired sleep on different body systems includes:7
Metabolic:
- Insulin resistance, increased diabetes risk.
- Impairment in growth hormone and muscle repair.
- Testosterone suppression and decreased libido.
- Ghrelin/leptin imbalance and increased appetite.
Cardiovascular:
- Increase in autonomic arousal.
- Hypertension.
- Increased risk for arrhythmia.
- Endothelial dysfunction.
- Increased risk of cardiovascular events.
Immune:
- Reduction in antibody production. ?Inflammatory cytokine production. ?Increased susceptibility to cold and infections.
Neurologic:
- Impairment of the glymphatic system (a perivascular system in the CNS responsible for waste elimination). ?Memory consolidation impairment.
Psychological:
- Increased depression risk.
Acute effects on mood, irritability, energy level, sense of wellbeing.
How to improve sleep
Sleep hygiene tips:7
- Aim to get between seven and nine hours of sleep.
- Have a consistent sleep time.
- Exercise regularly.
- Avoid late afternoon/evening naps and long naps.
- Avoid light exposure (electronics, etc) near bedtime.
- Limit caffeine consumption in the afternoon/evening.
- Limit alcohol consumption.
- Avoid large mixed meals and unhealthy foods near bedtime.
- Practice mindfulness techniques.
- Create a dark, cool, and quiet sleeping environment.
- Have a constant bedtime routine.
- Refrain from using the bed for non- sleep activities.
- Use a comfortable mattress, pillow, and bedding.
Summary
Fatigue is a common but often complex symptom with a wide range of potential physical, psychological and lifestyle-related causes. As it is frequently multifactorial, effective management requires a holistic approach that considers underlying conditions, sleep, mental wellbeing, medication use and nutritional status. Pharmacists are well placed to identify potential contributing factors, provide evidence-based advice, and facilitate appropriate referral where necessary.
Author: Dr Donna Cosgrove PhD. Donna’s overall aim is to improve patient outcomes through education. After graduating with a BSc in Pharmacy, she returned to university to complete a MSc in Neuropharmacology. This led to a PhD investigating the genetics of schizophrenia, followed by a postdoctoral research position in the same area. She has worked in hospital, research and community pharmacy settings and is currently a community pharmacist in Galway and a clinical writer.
References
1. Yoon JH, Park NH, Kang YE, Ahn YC, Lee EJ, Son CG. The demographic features of fatigue in the general population worldwide: a systematic review and meta- analysis. Frontiers in Public Health. 2023 Jul 28;11:1192121.
2. Kunasegaran K, Ismail AM, Ramasamy S, Gnanou JV, Caszo BA, Chen PL. Understanding mental fatigue and its detection: a comparative analysis of assessments and tools. PeerJ. 2023 Aug 23;11:e15744.
3. Stadje R, Dornieden K, Baum E, Becker A, Biroga T, Bösner S, Haasenritter J, Keunecke C, Viniol A, Donner-Banzhoff N. The differential diagnosis of tiredness: a systematic review. BMC Family Practice. 2016 Oct 20;17(1):147.
4. National Institute for Health and Care Excellence (NICE). Myalgic encephalomyelitis (or encephalopathy)/chronic fatigue syndrome: diagnosis and management [Internet]. London: NICE; 2021 Oct 29 [cited 2026 May 23]. (Clinical guideline; no. NG206). Available from: https://www.nice.org.uk/guidance/ng206.
5. Zlott DA, Byrne M. Mechanisms by which pharmacologic agents may contribute to fatigue. PM&R. 2010 May 1;2(5):451-5.
6. Tardy AL, Pouteau E, Marquez D, Yilmaz C, Scholey A. Vitamins and minerals for energy, fatigue and cognition: a narrative review of the biochemical and clinical evidence. Nutrients. 2020 Jan;12(1):228.
7. Baranwal N, Phoebe KY, Siegel NS. Sleep physiology, pathophysiology, and sleep hygiene. Progress in Cardiovascular Diseases. 2023 Mar 1;77:59-69.