Eamonn Brady MPSI reviews seborrheic dermatitis, including causes, those most commonly affected, and treatment strategies
Seborrhoeic dermatitis is a common chronic inflammatory skin condition that mainly affects areas of the body rich in sebaceous (oil-producing) glands. These areas include the scalp, face, ears, eyebrows, sides of the nose, beard area, chest and upper back. The condition typically presents with redness, flaking, greasy scale and irritation of the skin.
Although the term ‘seborrhoeic’ implies excessive oil production, increased sebum production is not always present in affected individuals. Instead, the condition appears to result from a complex interaction between skin oils, skin micro-organisms, inflammation, and an individual’s immune response.
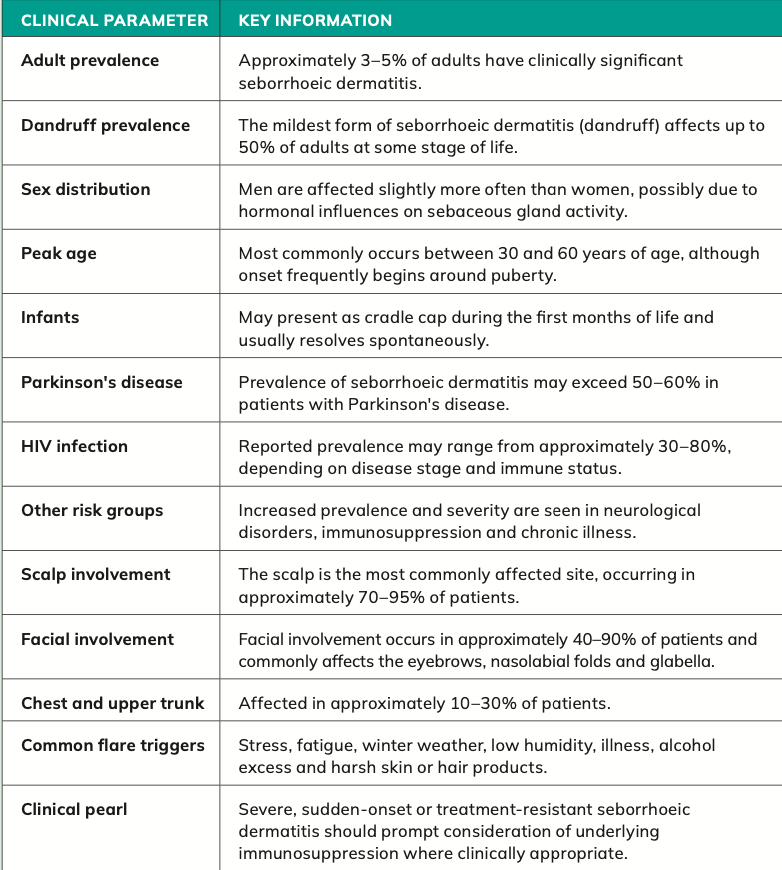
Seborrhoeic dermatitis is extremely common worldwide and affects people of all ethnic backgrounds. It is estimated that approximately 3-to-5 per cent of adults develop clinically significant seborrhoeic dermatitis, while mild dandruff, considered the mildest form of the condition, may affect up to 50 per cent of adults at some stage of life. Men are affected slightly more often than women, possibly due to hormonal influences on sebaceous gland activity.

Source: DermNet NZ. (n.d.). Seborrhoeic dermatitis (face). Available at: https://dermnetnz. org/topics/seborrhoeic-dermatitis (Accessed: 20 May 2025).
Who is affected?
The condition commonly develops during puberty when sebaceous gland activity increases under hormonal influence. Prevalence tends to peak during early adulthood and middle age, particularly between 30 and 60 years. However, seborrhoeic dermatitis can occur at any age, including infancy, where it is commonly presented as cradle cap. In older adults the condition may become less severe, although some individuals continue to experience persistent or recurrent symptoms throughout life.
Seborrhoeic dermatitis often follows a relapsing and remitting course, meaning symptoms improve and worsen over time. Many patients notice flare-ups during colder weather, particularly in autumn and winter when humidity levels fall and indoor heating dries the skin. Emotional stress, fatigue, illness and lack of sleep are also recognised triggers. Mechanical irritation from scratching, harsh soaps, over-washing, alcohol-based skincare products, and friction from clothing or protective headgear may worsen symptoms further.
Impact on quality of life and associated conditions Recent international guidance, including NICE recommendations and European dermatology guidance, increasingly recognises seborrhoeic dermatitis as more than simply a cosmetic problem. Persistent itching, visible facial scaling and scalp flaking can significantly affect self-confidence, social interaction and quality of life. Some patients report embarrassment, anxiety and reduced social confidence because of visible dandruff or facial redness.
Seborrhoeic dermatitis is also more common in certain medical conditions. Increased rates are seen in patients with Parkinson’s disease, HIV infection, depression, epilepsy and other neurological conditions. Prevalence may exceed 50 per cent in patients
with Parkinson’s disease. People with weakened immune systems may experience more severe or treatment- resistant disease. In patients with sudden severe onset or unusually resistant seborrhoeic dermatitis, clinicians may occasionally consider investigating for underlying immunosuppression.

Figure 2: Scalp seborrhoeic dermatitis
Source: DermNet NZ. (n.d.). Seborrhoeic dermatitis (scalp). Available at: https://dermnetnz. org/topics/seborrhoeic-dermatitis (Accessed: 20 May 2025).
Causes
Role of Malassezia species (yeast/fungus) and skin inflammation
The exact cause of seborrhoeic dermatitis remains incompletely understood, but current evidence suggests that several factors contribute to its development. Modern research indicates that the condition results from a combination
of increased sebaceous gland activity, overgrowth of naturally occurring skin yeasts, disruption of the skin barrier, and an exaggerated inflammatory response by the immune system.
One of the most important factors appears to involve Malassezia yeast (fungus) species. These fungi are naturally present on healthy human skin and usually cause no problems. However, in susceptible individuals, excessive growth of Malassezia species may triggerinflammation and scaling. The yeasts break down skin oils into irritating fatty acids, which can disrupt the skin barrier and provoke redness and irritation. Current evidence suggests seborrhoeic dermatitis results from an abnormal inflammatory response to Malassezia species rather than simple fungal overgrowth alone.
This theory is strongly supported by the effectiveness of antifungal treatments such as ketoconazole, ciclopirox and selenium sulphide, all of which reduce Malassezia levels on the skin and improve symptoms in many patients. Modern guidelines continue to recommend antifungal shampoos and creams as first- line treatment options for scalp and facial seborrhoeic dermatitis.
Sebaceous gland activity also plays a major role. Areas most affected by seborrhoeic dermatitis are typically those with the highest concentration of sebaceous glands. Hormonal changes that increase oil production, especially during puberty and early adulthood, may partly explain why the condition becomes more common after adolescence.
Genetic and environmental influences
Genetic susceptibility may also contribute. Some individuals appear genetically predisposed to developing inflammatory reactions to Malassezia species or skin oils. In addition, impaired skin barrier function may allow irritants and micro- organisms to penetrate the skin more easily, leading to chronic inflammation.
Environmental factors are increasingly recognised as important triggers. Cold weather, low humidity, stress and fatigue can all worsen symptoms. Dietary factors have also been explored, although evidence remains limited. Evidence linking diet and seborrhoeic dermatitis remains limited and inconsistent.
Certain medications may occasionally worsen seborrhoeic dermatitis, including lithium, interferon and some psychiatric medicines. Excess alcohol intake, smoking and chronic stress may also contribute to flare-ups in some patients.
Symptoms
Symptoms affecting the scalp and face
Seborrhoeic dermatitis typically presents with redness, flaking and scaling of the skin, often accompanied by itching, irritation or burning discomfort. The scales may appear white, yellow or greasy, depending on the severity and body area involved. Symptoms may vary considerably between individuals, ranging from mild dandruff, to widespread inflamed skin.
The scalp is the most commonly affected site. Patients may notice loose flakes on the scalp and clothing, itchy patches or diffuse scaling. In more severe cases, thick greasy plaques and marked inflammation may develop. Persistent scratching can occasionally lead to secondary bacterial infection, or temporary increased hair shedding may occasionally occur secondary to scalp inflammation and scratching.
Facial involvement is also very common. The sides of the nose, nasolabial folds, eyebrows, eyelids and the glabella area between the eyebrows are frequently affected. Redness and greasy scaling around the eyebrows and nose are particularly characteristic features. Some patients also develop scaling within the ears or behind the ears, where painful cracking may occasionally occur.
In men, seborrhoeic dermatitis often affects moustache and beard areas because facial hair traps oils and moisture, creating an environment favourable for Malassezia growth. Regular beard cleansing and, in some cases, shaving may help improve symptoms.
Symptoms in other body areas and infants
Less commonly, seborrhoeic dermatitis affects the chest, upper back, armpits and groin folds. In skin folds, the condition may appear more red and moist,
with less obvious scaling. Itching can sometimes become quite troublesome, particularly during warm weather or periods of sweating.
Infantile seborrhoeic dermatitis, commonly known as cradle cap, usually appears within the first few months of life. Thick, yellowish, greasy scales develop on the scalp and occasionally around the eyebrows or nappy area. Cradle cap is usually harmless, not contagious and often resolves spontaneously within several months. Cradle cap does not appear to cause discomfort in most infants. Current Irish and international guidance recommends gentle emollients and mild baby shampoos rather than aggressive scale removal.
Seborrhoeic dermatitis can occasionally resemble other skin conditions, including psoriasis, eczema, rosacea, fungal infections or lupus. Psoriasis tends to produce thicker, silvery scale and more sharply-defined plaques, while eczema is often associated with drier skin and stronger itch. In difficult cases, medical assessment may be required to confirm the diagnosis.
Although seborrhoeic dermatitis is not dangerous, it is a chronic condition with a tendency to recur. Long-term management often focuses on controlling symptoms and reducing flare-ups rather than achieving permanent cure. Modern treatment approaches aim to reduce inflammation, control overgrowth of Malassezia, and support restoration of the skin barrier while minimising irritation from overly-harsh products.
Diagnosis
Seborrhoeic dermatitis is usually diagnosed clinically through physical examination and assessment of symptom history. In most cases, no laboratory tests are required, particularly when the condition presents with its typical appearance and distribution. Healthcare professionals generally diagnose the condition based on the presence of greasy scaling, redness, and irritation affecting sebaceous gland-rich areas such as the scalp, eyebrows, sides of the nose, beard area and upper chest.
A detailed patient history is important. Questions regarding seasonal worsening, stress, fatigue, use of skincare products, occupational exposures, family history of skin disease, and response to previous treatments may assist diagnosis and help identify potential triggers.
Although diagnosis is usually straightforward, several skin conditions can closely resemble seborrhoeic dermatitis and may need to be excluded. Correct diagnosis is important because treatment approaches differ considerably between conditions.
Scalp differential diagnosis
On the scalp, seborrhoeic dermatitis must often be distinguished from psoriasis, atopic eczema and fungal or bacterial scalp infections. Psoriasis of the scalp typically produces thicker, more sharply defined plaques with silvery-white scale. The scaling is often drier and more adherent than in seborrhoeic dermatitis.
Psoriasis may also involve the elbows, knees and nails. In some patients, a condition known as ‘sebopsoriasis’ occurs, where features of both psoriasis and seborrhoeic dermatitis overlap.
Atopic dermatitis, or eczema, usually causes more intense itching and tends to occur in patients with a personal or family history of asthma, hay fever or allergic conditions. The skin is often drier and more sensitive than in seborrhoeic dermatitis.
Impetigo, a superficial bacterial skin infection, may occasionally resemble seborrhoeic dermatitis when crusting occurs on the scalp. However, impetigo generally produces honey-coloured crusts and may spread rapidly. It is more common in children.
Tinea capitis, a fungal scalp infection, may also need consideration, particularly in children or immuno-compromised adults. Hair loss, broken hairs and inflamed patches are more suggestive
of fungal infection than seborrhoeic dermatitis. Although uncommon in adults, tinea capitis should be considered in patients presenting with patchy alopecia, broken hairs or lymphadenopathy.
Facial differential diagnosis
Facial seborrhoeic dermatitis can resemble rosacea, psoriasis, contact dermatitis and lupus erythematosus.
Rosacea commonly causes redness across the cheeks and nose with visible blood vessels and sometimes acne-
like spots, but scaling tends to be less prominent than in seborrhoeic dermatitis. Periorificial dermatitis may occasionally be mistaken for facial seborrhoeic dermatitis, particularly in patients with a history of topical corticosteroid use.
Contact dermatitis may result from allergic or irritant reactions to cosmetics, skincare products, shaving products or occupational exposures. It often causes marked itching or burning and may be linked to the use of a new product.
Facial psoriasis generally produces more sharply-defined plaques with thicker scaling than seborrhoeic dermatitis. In persistent or atypical cases, clinicians may occasionally consider lupus erythematosus, particularly if photosensitivity or systemic symptoms are present.
Trunk differential diagnosis
When seborrhoeic dermatitis affects the chest or upper back, pityriasis versicolor and pityriasis rosea may need to be excluded.
Pityriasis versicolor is also associated with Malassezia species overgrowth and produces pale, dark or pink scaly patches on the trunk. Unlike seborrhoeic dermatitis, pigmentation changes are often more obvious.
Pityriasis rosea usually begins with a single ‘herald patch’, followed by multiple oval scaly lesions on the trunk in a characteristic distribution.
Additional investigations
Most patients do not require investigations. However, skin scrapings, fungal cultures or skin biopsy may occasionally be performed if the diagnosis is uncertain or symptoms fail to respond to standard treatment.
Modern dermatology guidance also recommends considering underlying conditions in patients with unusually severe or resistant seborrhoeic dermatitis. Particularly severe, extensive or treatment- resistant seborrhoeic dermatitis should prompt consideration of underlying immunosuppression, including HIV infection, especially where other risk factors or clinical features are present.
Dermoscopy is increasingly used by dermatologists to assist diagnosis in difficult cases. Dermoscopy is a non-invasive diagnostic technique that uses a specialised magnifying device with polarised light to enhance visual assessment of skin lesions and improve early detection of skin cancer. Characteristic findings of dermoscopy include diffuse scaling, arborising vessels and follicular changes, although diagnosis remains primarily clinical.
Impetigo, a superficial bacterial skin infection, may occasionally resemble seborrhoeic dermatitis when crusting occurs on the scalp
Treatment
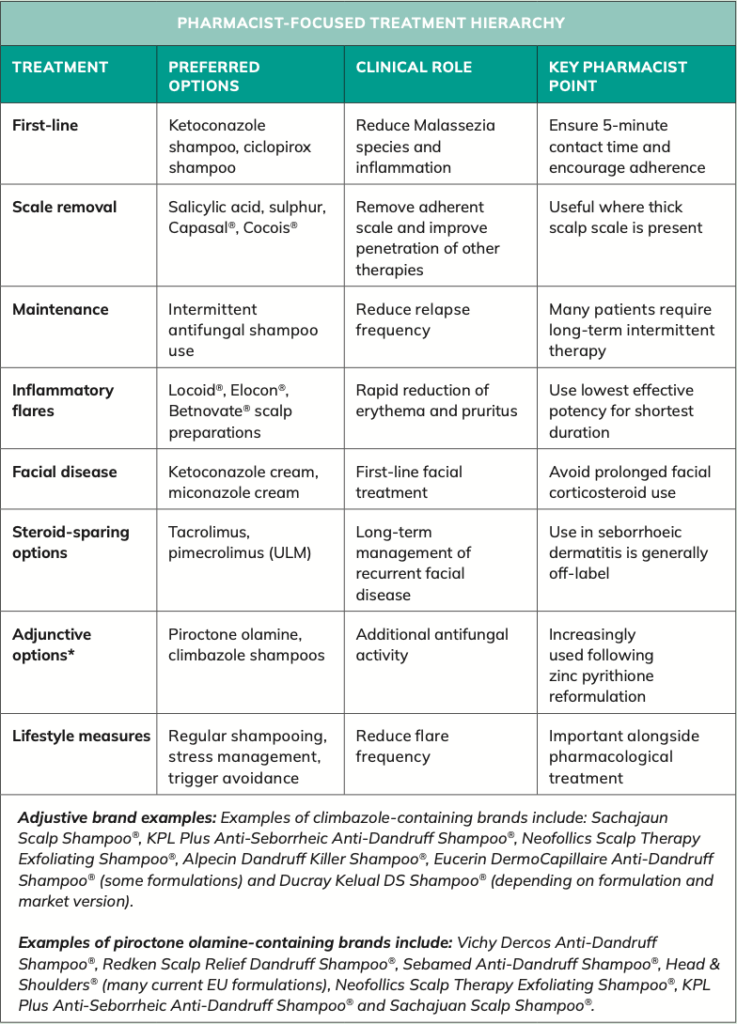
Seborrhoeic dermatitis is a chronic relapsing inflammatory skin disorder for which there is currently no permanent cure. However, modern therapeutic approaches can effectively control symptoms, reduce the frequency of flare- ups, and significantly improve quality of life for most patients. Current UK, European and international dermatology guidance emphasises a multifaceted treatment strategy aimed at reducing Malassezia species colonisation, controlling inflammation, removing excessive scale, and restoring normal skin barrier function. Pharmacists play an important role in identifying appropriate treatment options, promoting adherence and advising on long-term maintenance strategies.
Treatment should be individualised according to disease severity, body site involvement, and patient preference. While mild disease may respond adequately to over-the- counter products, moderate or severe disease often requires prescription therapies and ongoing maintenance treatment. Patients should be advised that seborrhoeic dermatitis frequently follows a chronic relapsing course, with symptoms commonly worsening during periods of stress, illness, fatigue, seasonal change or exposure to environmental triggers. As a result, many individuals require intermittent long- term treatment rather than short-term symptom control alone. This treatment section is split into two; seborrhoeic dermatitis of the scalp, and seborrhoeic dermatitis of the face.
Note: Several products discussed below are intermittently unavailable in Ireland. Where relevant, current availability and unlicensed alternatives are discussed under the individual product sections.
Seborrhoeic dermatitis of the scalp, including dandruff Dandruff represents the mildest and most common manifestation of scalp seborrhoeic dermatitis and affects a substantial proportion of the adult population. Although often regarded as a cosmetic concern, persistent dandruff can significantly impact confidence and quality of life. The primary goals of treatment are to reduce scaling, alleviate pruritus, suppress Malassezia proliferation, and minimise inflammation.
Regular shampooing remains the cornerstone of scalp management. Current guidance generally recommends frequent washing during active flare-ups, ranging from daily use to several times weekly, depending on disease severity and hair type. Patients should be counselled to leave medicated shampoos in contact with the scalp for at least five minutes before rinsing, as inadequate contact time is a common cause of treatment failure. Once satisfactory control is achieved, many patients can transition to maintenance therapy using medicated shampoos once or twice weekly.
Treatment shampoos generally fall into four principal categories:
- Keratolytic agents.
- Regulators of keratinisation.
- Antimicrobial agents.
- Antifungal agents.
Each group targets different aspects of disease pathophysiology and may be used alone or in combination, depending on symptom severity. In clinical practice, antifungal shampoos are increasingly regarded as first-line therapy because of their ability to directly target Malassezia species, which are believed to play a central role in disease development. However, keratolytic and keratinisation- regulating agents remain useful adjuncts, particularly in patients with substantial scale build-up.
Pharmacists should also reinforce the importance of realistic treatment expectations. While modern therapies are highly effective at controlling symptoms, recurrence is common when treatment is discontinued completely. Ongoing maintenance therapy, trigger avoidance and appropriate scalp care remain essential components of long-term disease management.
Keratolytic agents
Keratolytic agents play an important role in the management of scalp seborrhoeic dermatitis, particularly in patients with significant scale accumulation. These agents act by softening and loosening adherent scales, facilitating their removal from the scalp surface and improving the penetration of other topical treatments. By reducing excessive scale build-up, keratolytic preparations may also help decrease irritation, itching, and the physical barrier that can limit the effectiveness of antifungal therapies.
Salicylic acid remains one of the most commonly used keratolytic agents in clinical practice. It acts by disrupting the cohesion between corneocytes within the stratum corneum, thereby promoting desquamation and reducing the accumulation of thick scales. Salicylic acid is particularly useful in patients with substantial scalp scaling or in those with overlapping seborrhoeic dermatitis and psoriasiform features.
Salicylic acid remains one of the most commonly used keratolytic agents
in clinical practice
Sulphur is sometimes combined with salicylic acid because it possesses additional keratolytic and mild antimicrobial properties, potentially enhancing overall efficacy.
Examples available in Ireland include Capasal shampoo and Cocois ointment. Cocois contains a combination of coal tar, salicylic acid and sulphur, making it particularly useful in patients with stubborn, thick scalp scale. However, its requirement for prolonged contact time before shampooing can negatively affect adherence. The product may also be perceived as greasy and inconvenient compared with modern shampoo-based formulations.
Cocois has experienced intermittent supply shortages over the past two years and, at the time of writing (June 2026), remains unavailable through normal supply channels, with the expected return date ‘pending’. There are unlicensed versions available from companies like Uniphar and McDowells. Capasal shampoo has no supply issues currently.
Pharmacists should advise patients that excessive or prolonged use of keratolytic preparations may occasionally cause scalp irritation, dryness or erythema, particularly in individuals with sensitive skin or co-existing eczema. Careful patient selection and counselling remain important to maximise benefit while minimising adverse effects.
Regulators of keratinisation
Regulators of keratinisation aim to normalise the accelerated epidermal turnover that contributes to scale formation in seborrhoeic dermatitis. These agents can be useful as part of an overall treatment strategy, particularly in patients with recurrent dandruff or persistent scalp scaling.
Zinc pyrithione remains one of the most widely-recognised agents in this category and has historically been incorporated into numerous over- the-counter dandruff shampoos. In addition to regulating keratinocyte turnover, zinc pyrithione possesses antifungal activity against Malassezia species and may help reduce inflammation, scaling and pruritus. Products containing zinc pyrithione have included Head & Shoulders and a number of generic anti-dandruff shampoos available internationally.
However, the regulatory status and availability of zinc pyrithione-containing products have evolved significantly in recent years. Following safety assessments by European regulatory authorities, concerns were raised regarding potential reproductive toxicity based largely on animal data. As a result, zinc pyrithione was no longer approved for use in cosmetic products within the European Union from 2022 onwards. Consequently, many manufacturers reformulated anti-dandruff shampoos for the European market or replaced zinc pyrithione with alternative active ingredients such as piroctone olamine, climbazole, or selenium sulphide.
It is important for pharmacists to recognise that product availability may therefore vary considerably between jurisdictions. While zinc pyrithione- containing shampoos continue to be available in some non-EU markets, many products sold within Ireland and other EU countries have been reformulated. Pharmacists should therefore be aware that international treatment guidelines and product reviews may occasionally reference formulations that are no longer available in the Irish market.
Coal tar has historically been used in both psoriasis and seborrhoeic dermatitis because of its ability to suppress excessive epidermal proliferation and reduce scale formation. Tar preparations may also contribute indirectly to reductions in Malassezia colonisation by decreasing the amount of scale available on the scalp surface. Despite these benefits, use of coal tar has declined substantially because of cosmetic limitations, including staining, unpleasant odour and reduced patient acceptability.
Although some coal tar-containing products remain available, modern clinical guidance generally positions them as second-line or adjunctive therapies. Antifungal shampoos such as ketoconazole and ciclopirox are typically preferred because of stronger evidence supporting their efficacy and improved patient adherence. Nevertheless, selected patients with significant scaling may continue to derive benefit from coal tar-containing preparations, particularly when combined with keratolytic agents such as salicylic acid.
Antimicrobial agents
Selenium sulphide-containing shampoos have been used for many years in the treatment of seborrhoeic dermatitis and dandruff.
Their primary mechanism involves reducing the proliferation of Malassezia species on the scalp, thereby helping to reduce inflammation, flaking and pruritus. Although often classified as antimicrobial agents, selenium sulphide products also possess significant antifungal activity, which contributes to their clinical effectiveness in seborrhoeic dermatitis.
In addition to their role in seborrhoeic dermatitis, selenium sulphide preparations may also be used in the treatment of pityriasis versicolor caused by Malassezia species. Clinical studies have demonstrated that selenium sulphide can effectively reduce scalp scaling and itching, although some patients may find it less cosmetically acceptable than ketoconazole-based products.
Pharmacists should counsel patients regarding correct application techniques and potential adverse effects. Selenium sulphide shampoos should generally be left on the scalp for several minutes before rinsing thoroughly. Excessive use may lead to scalp irritation, dryness or increased sensitivity. Patients with chemically treated, coloured or grey hair should be advised that temporary hair discolouration may occasionally occur. Selsun shampoo was historically one of the best-known selenium sulphide preparations available in Ireland but has been withdrawn from the Irish market. Unlicensed alternatives remain available through specialist suppliers and wholesalers.
Antifungal agents
Antifungal shampoos are widely regarded as first-line therapy for moderate scalp seborrhoeic dermatitis because they directly target Malassezia species, believed to play a central role in disease pathogenesis. Their efficacy is supported by numerous clinical trials and international dermatology guidelines.
Ketoconazole remains one of the most extensively studied agents. It inhibits fungal ergosterol synthesis, disrupting fungal cell membrane integrity and reducing Malassezia colonisation. Nizoral 2% shampoo is widely used in Irish clinical practice and is frequently recommended by both pharmacists and dermatologists. Typical treatment regimens involve twice-weekly application during acute flare-ups, followed by intermittent maintenance therapy to reduce recurrence. Evidence suggests that regular maintenance use can significantly prolong remission periods. Relapse commonly occurs following treatment discontinuation, supporting the role of intermittent maintenance therapy in recurrent disease. Nizoral is available as a 120ml prescription-only pack with GMS reimbursement eligibility, and as a smaller over-the-counter pack.
Ciclopirox olamine represents another important antifungal option. Unlike ketoconazole, ciclopirox exhibits both antifungal and direct anti- inflammatory activity, a characteristic that may offer particular benefit in patients with prominent erythema and inflammatory disease. Clinical trials have demonstrated significant improvements in scaling, erythema and pruritus when compared with placebo. Comparative studies indicate that both ketoconazole and ciclopirox provide excellent efficacy, with treatment choice often influenced by patient preference, tolerability and availability. However, the main Irish brand, Stieprox, has been discontinued, although unlicensed alternatives remain available through a number of wholesalers.
Piroctone olamine and climbazole are increasingly encountered in modern anti-dandruff shampoos and have assumed greater importance following regulatory changes affecting zinc pyrithione-containing products within the European Union. Both agents possess antifungal activity against Malassezia species and are incorporated into a variety of cosmetic and pharmacy shampoo formulations.
Although the evidence base is less extensive than for ketoconazole and ciclopirox, they may be useful options in patients with mild-to-moderate dandruff or as part of maintenance treatment strategies.
From a pharmacist perspective, patient counselling is critical. Treatment failure is often related to inadequate contact time or poor adherence rather than lack of efficacy. Patients should therefore be encouraged to use products consistently and continue maintenance treatment where appropriate.
Topical corticosteroids and calcineurin inhibitors
Topical corticosteroids remain valuable options for short-term control of acute inflammatory flare-ups, particularly where marked erythema, irritation
or pruritus are present. Their anti- inflammatory effects can provide rapid symptomatic relief and improve patient comfort within a relatively short period.
Common scalp corticosteroid preparations available in Ireland include Locoid scalp application, Elocon scalp lotion, and Betnovate scalp application. Alcohol-based lotions, foams and gels are generally preferred for scalp use because they are easier
to apply through hair and dry rapidly following application.
Despite their effectiveness, corticosteroids should be used with caution. The lowest effective potency should be selected, and treatment duration kept as short as possible. Prolonged or inappropriate use may result in skin atrophy, telangiectasia, tachyphylaxis, rebound flare-ups and steroid dependence. Current UK, European and international dermatology guidance therefore recommends restricting use to short treatment courses during acute exacerbations.
Topical calcineurin inhibitors are discussed in greater detail under the section on facial seborrhoeic dermatitis. Although licensed primarily for atopic dermatitis, their use in seborrhoeic dermatitis is generally off-label. They provide useful steroid- sparing alternatives, particularly for recurrent disease affecting sensitive skin sites, and avoid the risk of skin- thinning associated with prolonged corticosteroid use.
Tea tree oil and natural remedies
Tea tree oil shampoos continue to be marketed for dandruff treatment. Tea tree oil possesses antifungal
and anti-inflammatory properties, and some studies suggest modest benefit in reducing scalp flaking. However, evidence remains limited and inconsistent. Tea tree oil may also cause allergic contact dermatitis in some individuals, particularly at higher concentrations. Current evidence-based guidelines do not recommend tea tree oil as first-line therapy, although some patients may find it beneficial as an adjunctive treatment. Pharmacists should remind patients that ‘natural’ does not necessarily equate to something being safer or more effective.
Other natural approaches sometimes explored include aloe vera, coconut oil, and honey-based preparations. While small studies suggest possible benefit, robust clinical evidence remains limited compared with established antifungal treatments.
Lifestyle and self-care advice
Patients should be advised that seborrhoeic dermatitis often improves with regular scalp care and trigger avoidance.
Helpful measures include:
- Regular shampooing.
- Avoiding harsh hair products.
- Managing stress levels.
- Reducing scratching.
- Maintaining good sleep habits.
- Limiting excessive alcohol intake where relevant.
Many patients benefit from alternating medicated shampoos with gentle non-medicated shampoos to reduce scalp irritation. Some patients also report improvement during periods of moderate sunlight exposure, although excessive ultraviolet exposure should not be recommended because of the associated risk of skin cancer. Education is important because many people mistakenly believe dandruff reflects poor hygiene. In reality, seborrhoeic dermatitis is an inflammatory skin condition and not caused by uncleanliness.
Facial seborrhoeic dermatitis
Although the scalp is the most commonly affected site in seborrhoeic dermatitis, facial involvement is also extremely common and frequently presents unique management challenges. Scalp involvement has been reported in approximately 70-to-95 per cent of patients with seborrhoeic dermatitis, while facial involvement has been reported in approximately 40-to-90 per cent of patients. These figures vary considerably between studies because of differences in patient populations, disease severity and diagnostic criteria. Nevertheless, the face remains the second-most commonly affected anatomical site, and many patients experience concurrent scalp and facial disease.
Because facial seborrhoeic dermatitis affects such a substantial proportion of patients and often
has a disproportionate impact on quality of life, it warrants separate discussion. Facial lesions are more visible than scalp involvement and may
Facial seborrhoeic dermatitis most commonly affects the nasolabial folds, eyebrows, glabella, beard area, and external ear canals
be associated with embarrassment,
reduced self-confidence and social anxiety. In addition, the thinner skin of the face, particularly around the eyelids and nasolabial folds, requires a more cautious therapeutic approach than the scalp.
Many of the treatments discussed in the previous sections, including antifungal agents and anti-inflammatory therapies, also play an important role in the management of facial seborrhoeic dermatitis. However, treatment selection, duration of therapy and
safety considerations differ sufficiently to justify separate review. Particular attention must be paid to minimising long-term corticosteroid exposure and selecting appropriate steroid-sparing alternatives for recurrent disease affecting sensitive facial skin.
Facial seborrhoeic dermatitis most commonly affects the nasolabial folds, eyebrows, glabella, beard area, and external ear canals. Eyelid involvement may also occur and can present as seborrhoeic blepharitis, characterised by erythema, irritation and scaling along the eyelid margins.
Antimicrobial and antifungal agents
Topical antifungal therapy is generally regarded as first-line treatment for facial seborrhoeic dermatitis. Ketoconazole 2% cream has been extensively studied and remains one of the most commonly recommended options. By reducing Malassezia species colonisation and associated inflammation, ketoconazole can effectively reduce erythema, scaling and pruritus. Treatment is typically applied once or twice daily during flare- ups and may subsequently be used intermittently as maintenance therapy in patients with recurrent disease.
Miconazole cream may also be effective, particularly where secondary yeast colonisation is suspected. Although the evidence base is less extensive than for ketoconazole, miconazole possesses both antifungal and some antibacterial activity and remains a useful treatment option in clinical practice.
Corticosteroids, keratolytic and keratinisation-regulating therapies
Low-potency topical corticosteroids such as hydrocortisone 1% cream may be used for short periods where significant inflammation, erythema or itching are present. However, because facial skin is more susceptible to corticosteroid- related adverse effects, treatment duration should generally be limited to short courses. Prolonged use may result in skin atrophy, telangiectasia, steroid- induced rosacea, and rebound flare-ups.
For patients with recurrent disease requiring repeated treatment courses, topical calcineurin inhibitors have become increasingly important steroid- sparing alternatives. Tacrolimus ointment and pimecrolimus (ULM in Ireland) cream reduce inflammation by inhibiting T-cell activation and cytokine release without causing skin thinning. Although their use in seborrhoeic dermatitis is generally off-label, a growing body of evidence supports their effectiveness, particularly for long-term management of facial disease.
Calcineurin inhibitors may be especially useful for involvement of sensitive areas such as the eyelids, nasolabial folds and retroauricular regions where repeated corticosteroid exposure is undesirable. Patients should be advised that transient burning or stinging may occur during the first few days of treatment, although this usually improves with continued use.
Management of seborrhoeic blepharitis often requires a combination of eyelid hygiene measures and pharmacological treatment. Gentle cleansing of the eyelid margins using warm compresses and lid-cleaning products may help remove scale and reduce irritation. More persistent cases may require referral to an ophthalmologist or dermatologist.
From a pharmacist perspective, patient counselling remains essential. Patients should be informed that seborrhoeic dermatitis is a chronic relapsing condition and that recurrence is common following treatment discontinuation. Long-term disease control is therefore often achieved through intermittent maintenance therapy, trigger avoidance and appropriate skin care, rather than continuous treatment.
Disclaimer: Brands mentioned in this article are meant as examples only and not meant as preference to other brands.
Written by Eamonn Brady (Pharmacist). Whelehans Pharmacies, 38 Pearse St and Clonmore, Mullingar. Tel 04493 34591 (Pearse St) or 04493 10266 (Clonmore). www.whelehans.ie
References
- Health Products Regulatory Authority (HPRA) (2025) Ketoconazole 2% Shampoo Summary of Product Characteristics. Dublin: HPRA.
- Health Products Regulatory Authority (HPRA) (2025) Hydrocortisone 1% Cream Summary of Product Characteristics. Dublin: HPRA.
- Health Products Regulatory Authority (HPRA) (2025) Elocon Scalp Lotion Summary of Product Characteristics. Dublin: HPRA.
- Health Products Regulatory Authority (HPRA) (2025) Locoid Scalp Application Summary of Product Characteristics. Dublin: HPRA.
- Health Products Regulatory Authority (HPRA) (2025) Betnovate Scalp Application Summary of Product Characteristics. Dublin: HPRA.
- Pharmaceutical Society of Ireland (PSI) (2024) Guidance for Pharmacists on Patient Counselling and Self-Care Advice. Dublin: PSI.
- HSE (2024) Skin Conditions and Self-Care Ad- vice. Dublin: Health Service Executive.
- HSE National Clinical Programme for Dermatol- ogy (2024) Dermatology Care Pathways. Dublin: Health Service Executive.
- Medicines Information Centre, St James’s Hospital (2024) Medicines Q&A: Topical Treatments for Seb- orrhoeic Dermatitis. Dublin: St James’s Hospital.
- Department of Health (Ireland) (2024) Sláin- tecare and Integrated Care for Chronic Disease Management. Dublin: Department of Health.
- Borda, LJ and Wikramanayake, TC (2015). ‘Seb- orrheic dermatitis and dandruff: a comprehen- sive review’, Journal of Clinical and Investigative Dermatology, 3(2), pp. 1–22.
- Clark GW, Pope SM and Jaboori KA (2015). ‘Di- agnosis and treatment of seborrheic dermatitis’, American Family Physician, 91(3), pp. 185–190. • Dessinioti C, and Katsambas A (2013). ‘Seb- orrheic dermatitis: etiology, risk factors and treatments’, Clinics in Dermatology, 31(4), pp. 343–351.
- Gupta AK, and Versteeg SG (2017). ‘Topical treatment of facial seborrheic dermatitis: a systematic review’, American Journal of Clinical Dermatology, 18(2), pp. 193–213.
- Gupta AK, Madzia SE, and Batra R (2004). ‘Eti- ology and management of seborrheic dermatitis’, Dermatology, 208(2), pp. 89–93.
- National Institute for Health and Care Excellence (NICE) (2025) Seborrhoeic Dermatitis: Clinical Knowledge Summary. London: NICE.
- European Dermatology Forum (EDF) (2024) European Guidance for the Management of Seb- orrhoeic Dermatitis. Brussels: EDF.
- American Academy of Dermatology (AAD) (2024). Seborrheic Dermatitis: Diagnosis and Treatment. Rosemont, IL: AAD.
- UpToDate (2026) Seborrheic Dermatitis in Ad- olescents and Adults: Treatment and Prognosis. Waltham, MA: UpToDate.
- Ring J et al (2012) ‘Guidelines for treatment of seborrhoeic dermatitis’, Journal of the European Academy of Dermatology and Venereology, 26(1), pp. 1–8.
- Turner GA, and Hoptroff M (2014). ‘Dandruff and seborrhoeic dermatitis: the contribution of Malasse- zia species’, Journal of Investigative Dermatology Symposium Proceedings, 17(2), pp. 16–18.
- Wu Y, Lin Y, and Zhang J (2022). ‘Advances in the understanding and management of seborrheic dermatitis’, Dermatologic Therapy, 35(9), pp. 1–12.
References for table 1 and 2
- Borda LJ, and Wikramanayake TC (2015). ‘Seb- orrheic dermatitis and dandruff: a comprehen- sive review’, Journal of Clinical and Investigative Dermatology, 3(2), pp. 1–22.
- Dessinioti C, and Katsambas A (2013). ‘Seb- orrheic dermatitis: etiology, risk factors and treatments’, Clinics in Dermatology, 31(4), pp. 343–351.