






Eamonn Brady MPSI synopsises psychosomatic illness, including presentation, causes, and complications
What is psychosomatic illness
Psychosomatic illness describes the interaction between psychological processes and physical symptom expression, whereby patients experience genuine physical symptoms that are not fully explained by identifiable organic pathology. The terminology has evolved significantly in recent years, and contemporary classification, particularly within DSM-5, now refers to these conditions as somatic symptom and related disorders (SSRDs), reflecting a shift away from the older ‘somatoform’ terminology and a greater emphasis on patient experience rather than absence of disease.
In this article, the term psychosomatic illness is used broadly to reflect conditions now classified as somatic symptoms and related disorders.
Presentation in practice
From a pharmacy and primary care perspective, these conditions are both highly prevalent and commonly encountered in everyday practice. Patients often present with persistent and distressing physical symptoms.
These presentations often lead to repeated consultations, ongoing investigations, and escalating medicine use without clear clinical benefit.
Clinical context
Clinically, psychosomatic illness may be broadly considered within three overlapping contexts. Firstly, where physical and psychiatric illness coexist and interact. Secondly, where psychological distress develops as a consequence of chronic physical illness. Thirdly, in primary somatic symptom disorders, where psychological factors manifest predominantly through physical symptoms, often without an identifiable organic cause.
Epidemiology and importance
Epidemiologically, these conditions are more commonly reported in females and frequently present before mid-adulthood, although they may occur at any stage of life. Risk is increased in individuals with a history of trauma, chronic stress exposure, or co-morbid mental health conditions such as anxiety or depression.
Importantly, symptoms are neither fabricated nor intentional. Emerging neurobiological evidence suggests altered central processing of pain and bodily signals, reinforcing that these are legitimate and complex clinical presentations requiring appropriate recognition and management.
For pharmacists, early identification is essential in improving patient outcomes and reducing inappropriate medication use.
Symptoms
These symptoms can significantly impair day-to-day functioning and quality of life.
Common physical presentations
Common presentations encountered in pharmacy practice include chronic pain, such as musculoskeletal pain or recurrent headaches, gastrointestinal symptoms including nausea, bloating, diarrhoea, or IBS-type symptoms, as well as fatigue and reduced energy levels. Cardiopulmonary complaints are also frequently reported, particularly palpitations, chest discomfort, or breathlessness, which may prompt repeated reassurance-seeking behaviour.
Cognitive and behavioural features
In addition to physical symptoms, patients frequently exhibit characteristic cognitive and behavioural features. These include excessive health-related anxiety, persistent worry about having a serious illness, repeated checking or monitoring of symptoms, and frequent GP visits or pharmacy consultations. Patients may also demonstrate dissatisfaction with reassurance or normal test results, often feeling that their concerns have not been fully addressed.
Recognised subtypes
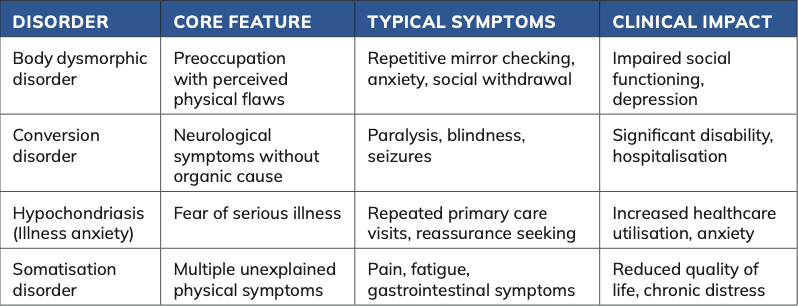
Several recognised subtypes fall within this spectrum. Body dysmorphic disorder involves a preoccupation with perceived defects in appearance, which can lead to distress and inappropriate use of cosmetic or over-the-counter products. Functional neurological disorder, also known as conversion disorder, presents with neurological symptoms such as weakness, seizures, or sensory loss in the absence of an organic cause. Illness anxiety disorder is characterised by a persistent fear of serious illness despite reassurance, often resulting in repeated consultations. Somatic symptom disorder involves multiple physical complaints accompanied by significant psychological overlay.
Pharmacy presentation patterns
In pharmacy practice, these patients may present through repeated OTC requests, poor adherence to prescribed treatments, or frequent switching between therapies. Medication use patterns are often inconsistent, and there may be a tendency towards increased use of symptomatic treatments. Careful assessment is essential to ensure that underlying organic pathology is not overlooked while also recognising the broader psychosomatic context.
Potential complications of psychosomatic illness
As outlined in the previous section on symptom presentation, failure to recognise psychosomatic illness early can lead to a range of significant clinical, psychological, and social complications. These consequences often develop gradually and
Illness anxiety disorder is characterised by a persistent fear of serious illness despite reassurance
may become entrenched if patterns of healthcare use and treatment are not addressed appropriately.
Healthcare system impact
From a healthcare system perspective, patients may undergo repeated investigations and specialist referrals with limited clinical benefit. This can result in increased healthcare utilisation, unnecessary diagnostic procedures, and escalating costs, while also exposing patients to avoidable interventions that may carry their own risks.
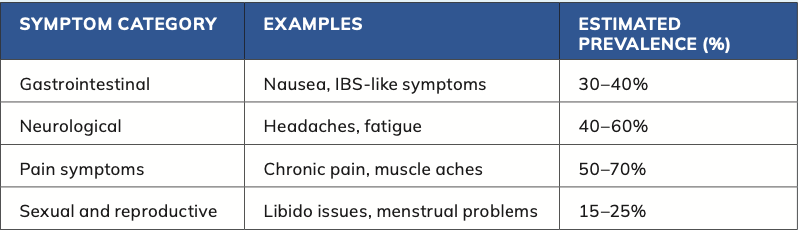
Table 1: Prevalence and symptom distribution in psychosomatic illness
Clinical risks
Clinical complications are important in pharmacy practice. Polypharmacy is common, often driven by attempts to manage persistent symptoms without addressing the underlying psychosomatic component. This increases the risk of adverse drug reactions, drug interactions, and reduces overall treatment effectiveness. There is also a recognised risk of dependence on medications such as analgesics or benzodiazepines, particularly where these are used for symptomatic relief over prolonged periods. In addition, untreated psychosomatic illness can contribute to the development or worsening of anxiety and depressive disorders, further compounding symptom burden, and functional impairment.
Psychosocial impact
Psychosocial consequences are equally significant. Patients may experience a reduced quality of life, with increasing social withdrawal and isolation. Occupational functioning can be affected, leading to absenteeism or reduced productivity, while personal relationships may become strained due to ongoing health concerns and emotional distress.
Risk considerations
Of particular concern is the increased risk of self-harm and suicidal ideation, especially in individuals with co-morbid mental health conditions. This highlights the importance of a holistic and proactive approach to management.
Role of the pharmacist
Pharmacists are well positioned to identify early warning signs in everyday practice. These may include frequent presentations with unexplained or recurrent symptoms, repeated OTC purchases for similar complaints, escalating or inappropriate medicine use, and visible signs of psychological distress.
Early intervention
Early recognition, combined with appropriate intervention and referral where necessary, can significantly improve patient outcomes, reduce unnecessary healthcare utilisation, and minimise long-term morbidity associated with psychosomatic illness.
Causes
Following on from the potential complications outlined previously, understanding the underlying causes of psychosomatic illness is essential in guiding effective management and patient support. The aetiology is multifactorial, involving a complex interplay between biological, psychological, and social factors, often referred to as the biopsychosocial model.
Biological factors
Biological contributors include a genetic predisposition, as well as alterations in the central processing of pain and somatic signals. Patients may have heightened sensitivity to normal bodily sensations, which are perceived as distressing or pathological. Dysregulation of the hypothalamic–pituitary–adrenal (HPA) axis also plays a role, particularly in individuals exposed to chronic stress, leading to sustained physiological responses that can manifest as physical symptoms.
Psychological factors
Psychological factors are central to the development of psychosomatic illness.
A history of trauma, including physical, emotional, or sexual abuse, is strongly associated with increased risk. Chronic stress, maladaptive coping strategies, and difficulty recognising or expressing emotions (alexithymia), can all contribute to the persistence and severity of symptoms. In many cases, physical symptoms represent an expression of unresolved psychological distress.
Social influences
Social influences further shape the presentation and progression of these conditions. Socioeconomic stressors, such as financial difficulty or job insecurity, can exacerbate symptoms. Family dynamics and levels of social support are also important, as is the broader cultural context in which illness is perceived and managed. Cultural beliefs may influence how patients interpret symptoms and when they seek medical care.
Early life factors
Adverse childhood experiences are particularly significant, with robust evidence linking early life stress to increased risk of psychosomatic illness in adulthood. These early experiences can affect both psychological resilience and biological stress responses.
Triggers
In addition to these underlying factors, specific triggers may precipitate symptom onset. These often include acute life events such as bereavement, physical illness, or major personal change, which may overwhelm an individual’s coping capacity.
Pharmacy perspective
For pharmacists, an awareness of these contributing factors supports a more empathetic and holistic approach to patient care. Recognising that symptoms arise from complex interactions rather than a single cause helps avoid dismissal and promotes more appropriate guidance, reassurance, and referral where necessary.
Treatment
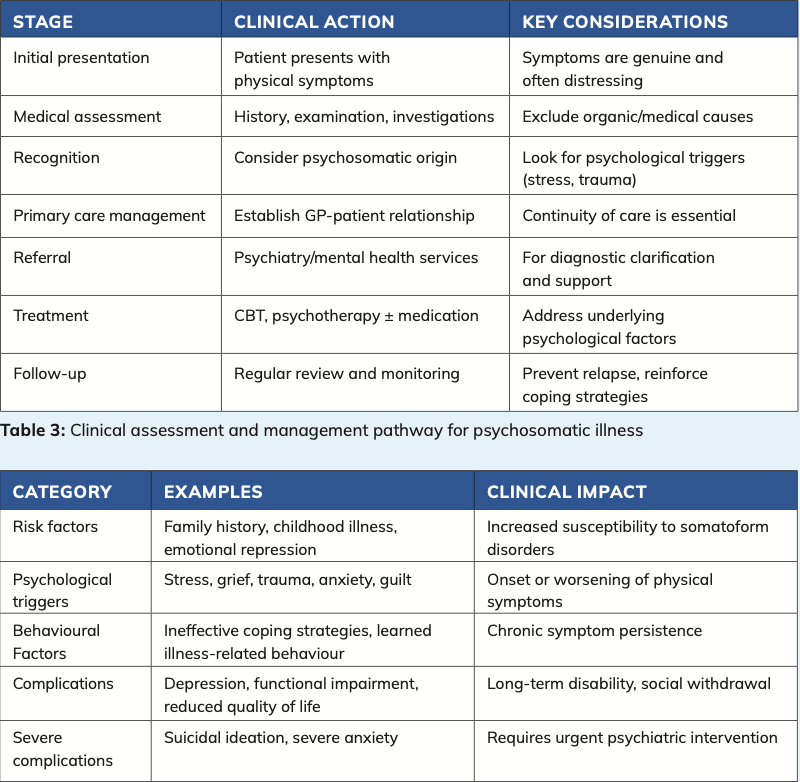
Continuity of care
A key principle is the establishment of a consistent and trusting relationship with a primary healthcare provider, typically the GP. Regular, planned follow-up appointments are more effective than reactive consultations, as they help reduce unnecessary healthcare utilisation while providing reassurance and a clear framework for ongoing management.
Psychological therapies
Psychological therapies are considered first-line treatment. Cognitive behavioural therapy (CBT) has the strongest evidence base and is effective in helping patients understand the link between thoughts, emotions, and physical symptoms. Mindfulness-based therapies and structured stress management approaches may also provide benefit, particularly in patients with high levels of anxiety or chronic stress.
Pharmacological treatment
Pharmacological treatment plays a more limited but still significant role and is generally directed at co- morbid conditions rather than the psychosomatic symptoms themselves. Selective serotonin reuptake inhibitors (SSRIs) or serotonin–noradrenaline reuptake inhibitors (SNRIs) may be used in the management of anxiety and depression, while low-dose tricyclic antidepressants can be beneficial in chronic pain syndromes.
Role of the pharmacist
From a pharmacy perspective, there are key responsibilities. Pharmacists are well placed to identify inappropriate or escalating medication use, particularly where patients are seeking repeated symptomatic relief. Supporting medication adherence, where appropriate, remains important, as does monitoring for potential drug interactions and adverse effects. Providing clear patient education and reassurance can help reduce anxiety and improve overall treatment outcomes.
Symptomatic treatment considerations
Symptomatic treatments may be used in the short term; however, these should be reviewed regularly to avoid long-term dependence or unnecessary polypharmacy. Encouraging a gradual shift towards non-pharmacological strategies is essential.
Non-pharmacological strategies
Non-pharmacological interventions are central to long-term management. These include sleep optimisation, regular physical activity, and the use of stress reduction techniques. Lifestyle interventions can significantly improve both physical and psychological wellbeing when implemented consistently.
Referral
Referral to mental health services should be considered in cases where symptoms are persistent, severe, or associated with significant psychological distress.
References
1. Barsky, AJ and Borus, JF (1999). Functional somatic syndromes. Annals of Internal Medi- cine, 130(11), pp.910–921.
2. Burton, C (2003). Beyond somatisation: a review of the understanding and treatment of medically unexplained physical symptoms (MUPS). British Journal of General Practice, 53(488), pp.231–239.
3. Deary, V, Chalder, T and Sharpe, M (2007). The cognitive behavioural model of medical- ly unexplained symptoms: a theoretical and empirical review. Clinical Psychology Review, 27(7), pp.781–797.
4. Dimsdale, JE and Creed, F (2009). The proposed diagnosis of somatic symptom disorders in DSM-5. Journal of Psychosomatic Research, 66(6), pp.473–476.
5. Fink, P and Schröder, A (2010). One single diagnosis, bodily distress syndrome, suc- ceeded to capture 10 diagnostic categories of functional somatic syndromes. Journal of Psychosomatic Research, 68(5), pp.415–426.
6. Hatcher, S. and Arroll, B. (2008). As- sessment and management of medically unexplained symptoms. BMJ, 336(7653), pp.1124–1128. Henningsen, P, Zipfel, S, and Herzog, W (2003). Management of functional somatic syndromes. The Lancet, 362(9385), pp.946–955.
7. Katon, W, Lin, EHB and Kroenke, K (2007). The association of depression and anxiety with medical symptom burden in patients with chronic medical illness. General Hospital Psychiatry, 29(2), pp.147–155.
8. Kirmayer, LJ and Robbins, JM (1991). Three forms of somatization in primary care. Journal of Nervous and Mental Disease, 179(11), pp.647–655.
9. Mayou, R, Kirmayer, LJ, Simon, G, Kroen- ke, K, and Sharpe, M (2005). Somatoform disorders: time for a new approach in DSM-5. American Journal of Psychiatry, 162(5), pp.847–855.
10. Olde Hartman, TC, Borghuis MS, Lucassen, PLBJ, van de Laar, FA, Speckens, AEM and van Weel, C (2009). Medically unexplained symp- toms, somatisation disorder, and hypochondri- asis: course and prognosis. British Journal of Psychiatry, 195(1), pp.70–75.
11. Rief, W and Broadbent, E (2007). Ex- plaining medically unexplained symptoms — models and mechanisms. Clinical Psychology Review, 27(7), pp.821–841.
12. Sharpe, M and Mayou, R (2004). Soma- toform disorders: a help or hindrance to good patient care? British Journal of Psychiatry, 184(6), pp.465–467.
13. Smith, RC, Dwamena, FC and Grover, M (2013). Behavioural medicine in primary care: a practical guide. New York: McGraw-Hill.
14. Stone, J, Carson, A, and Sharpe, M (2005). Functional symptoms and signs in neurology: assessment and diagnosis. Journal of Neurol- ogy, Neurosurgery & Psychiatry, 76(suppl 1), pp.i2–i12.
15. Toft, T, Fink, P, Oernboel, E, Christensen, K and Frostholm, L (2005). Mental disorders in primary care: prevalence and co-morbidity among disorders. Psychological Medicine, 35(8), pp.1175–1184.
16. Van Dessel, N, den Boeft, M, van der Wouden, JC, Kleinstäuber, M, Leone, SS, Terluin, B, Numans, ME and van der Horst, HE (2014). Non-pharmacological interven- tions for somatoform disorders and medically unexplained physical symptoms. Cochrane Database of Systematic Reviews, (11).
17. Wessely, S, Nimnuan, C and Sharpe, M (1999). Functional somatic syndromes: one or many? The Lancet, 354(9182), pp.936–939.
18. White, P.D. (2005). What causes chronic fatigue syndrome? BMJ, 330(7492), pp.122–123.
19.World Health Organization (2019). Interna- tional classification of diseases 11th revision (ICD-11). Geneva: WHO.
20. Abbass, A, Kisely, S and Kroenke, K (2009). Short-term psychodynamic psychotherapy for somatic disorders. Psychotherapy and Psycho- somatics, 78(5), pp.265–274.
21. Allen, LA, Woolfolk, RL, Escobar, JI, Gara, MA and Hamer, RM (2006). Cognitive-be- havioral therapy for somatization disorder. Archives of Internal Medicine, 166(14), pp.1512–1518.
22. Creed, FH (2006). The relationship be- tween psychosocial parameters and outcome in irritable bowel syndrome. American Journal of Medicine, 119(1), pp.S39–S44.
23. Escobar, JI, Gara, M, Diaz-Martinez, AM, Interian, A, Warman, M, and Allen, LA (2007). Effectiveness of a time-limited cognitive behavior therapy for medically unexplained symptoms. Journal of Consulting and Clinical Psychology, 75(5), pp.812–823.
24. Lipsitt, DR (2001). Somatization: the concept and its clinical application. American Journal of Psychiatry, 158(6), pp.859–867.
References/sources specific to table 1-4
TABLE 1
• Creed, F and Barsky, A (2004).
A systematic review of the epidemiology of somatisation disorder. Journal of Psychosomatic Research.
• Kroenke, K (2003). Patients presenting with somatic complaints: epidemiology and management. International Journal of Methods in Psychiatric Research.
• NICE guidance on medically unexplained symptoms and somatic symptom disorders.
• American Psychiatric Association (2013). DSM-5. Washington, DC.
TABLE 2
• American Psychiatric Association (2013). Diagnostic and Statistical Manual of Mental Disorders (DSM- 5). Washington, DC.
• NICE guidance on medically unexplained symptoms and somatic symptom disorders.
• Creed, F, Henningsen, P.
and Fink, P (2011). Medically unexplained symptoms, somatisation, and bodily distress. Cambridge University Press.
• Kroenke, K and Mangelsdorff, A (1989). Common symptoms in ambulatory care. American Journal of Medicines.
TABLE 3
• NICE guidance on medically unexplained symptoms and somatic symptom disorders.
• Sharpe, M et al (2011). Management of medically unexplained symptoms. BMJ.
• Creed, F and Barsky, A (2004). A systematic review of somatisation disorder. Journal of Psychosomatic Research.
• Royal College of Psychiatrists (2020). Medically unexplained symptoms guidance.
TABLE 4
• NICE guidance on medically unexplained symptoms and somatic symptom disorders.
• American Psychiatric Association (2013). DSM-5. Washington, DC.
• Henningsen, P. et al. (2007). Management of functional somatic syndromes. Lancet.
• Sharpe, M., and Carson, A. (2001). Unexplained somatic symptoms, functional syndromes, and somatisation. BMJ.






